Related Research Articles
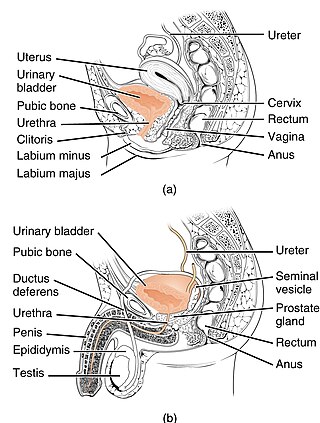
The urethra is the tube that connects the urinary bladder to the urinary meatus, through which placental mammals urinate and ejaculate. In non-mammalian vertebrates, the urethra also transports semen but is separate from the urinary tract.
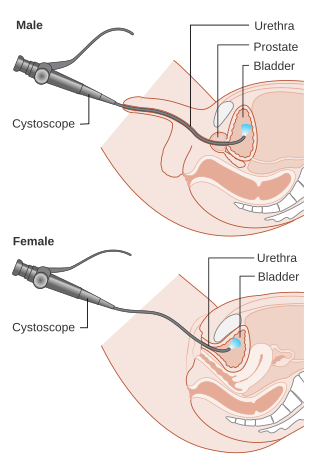
Cystoscopy is endoscopy of the urinary bladder via the urethra. It is carried out with a cystoscope.
Urinary incontinence (UI), also known as involuntary urination, is any uncontrolled leakage of urine. It is a common and distressing problem, which may have a large impact on quality of life. Urinary incontinence is common in older women and has been identified as an important issue in geriatric health care. The term enuresis is often used to refer to urinary incontinence primarily in children, such as nocturnal enuresis. UI is an example of a stigmatized medical condition, which creates barriers to successful management and makes the problem worse. People may be too embarrassed to seek medical help, and attempt to self-manage the symptom in secrecy from others.

Retrograde ejaculation occurs when semen which would be ejaculated via the urethra is redirected to the urinary bladder. Normally, the sphincter of the bladder contracts before ejaculation, inhibiting urination and preventing a reflux of semen into the bladder. The semen is forced to exit via the urethra, the path of least resistance. When the bladder sphincter does not function properly, retrograde ejaculation may occur. It can also be induced deliberately by a male as a primitive form of male birth control or as part of certain alternative medicine practices. The retrograde-ejaculated semen is excreted from the bladder during the next urination.

Urinary retention is an inability to completely empty the bladder. Onset can be sudden or gradual. When of sudden onset, symptoms include an inability to urinate and lower abdominal pain. When of gradual onset, symptoms may include loss of bladder control, mild lower abdominal pain, and a weak urine stream. Those with long-term problems are at risk of urinary tract infections.

The cystocele, also known as a prolapsed bladder, is a medical condition in which a woman's bladder bulges into her vagina. Some may have no symptoms. Others may have trouble starting urination, urinary incontinence, or frequent urination. Complications may include recurrent urinary tract infections and urinary retention. Cystocele and a prolapsed urethra often occur together and is called a cystourethrocele. Cystocele can negatively affect quality of life.

Radical retropubic prostatectomy is a surgical procedure in which the prostate gland is removed through an incision in the abdomen. It is most often used to treat individuals who have early prostate cancer. Radical retropubic prostatectomy can be performed under general, spinal, or epidural anesthesia and requires blood transfusion less than one-fifth of the time. Radical retropubic prostatectomy is associated with complications such as urinary incontinence and impotence, but these outcomes are related to a combination of individual patient anatomy, surgical technique, and the experience and skill of the surgeon.

Stress incontinence, also known as stress urinary incontinence (SUI) or effort incontinence is a form of urinary incontinence. It is due to inadequate closure of the bladder outlet by the urethral sphincter.
In urology, voiding cystourethrography (VCUG) is a frequently performed technique for visualizing a person's urethra and urinary bladder while the person urinates (voids). It is used in the diagnosis of vesicoureteral reflux, among other disorders. The technique consists of catheterizing the person in order to fill the bladder with a radiocontrast agent, typically diatrizoic acid. Under fluoroscopy the radiologist watches the contrast enter the bladder and looks at the anatomy of the patient. If the contrast moves into the ureters and back into the kidneys, the radiologist makes the diagnosis of vesicoureteral reflux, and gives the degree of severity a score. The exam ends when the person voids while the radiologist is watching under fluoroscopy. Consumption of fluid promotes excretion of contrast media after the procedure. It is important to watch the contrast during voiding, because this is when the bladder has the most pressure, and it is most likely this is when reflux will occur. Despite this detailed description of the procedure, at least as of 2016 the technique had not been standardized across practices.
Neurogenic bladder dysfunction, often called by the shortened term neurogenic bladder, refers to urinary bladder problems due to disease or injury of the central nervous system or peripheral nerves involved in the control of urination. There are multiple types of neurogenic bladder depending on the underlying cause and the symptoms. Symptoms include overactive bladder, urinary urgency, frequency, incontinence or difficulty passing urine. A range of diseases or conditions can cause neurogenic bladder including spinal cord injury, multiple sclerosis, stroke, brain injury, spina bifida, peripheral nerve damage, Parkinson's disease, multiple system atrophy or other neurodegenerative diseases. Neurogenic bladder can be diagnosed through a history and physical as well as imaging and more specialized testing. In addition to symptomatic treatment, treatment depends on the nature of the underlying disease and can be managed with behavioral changes, medications, surgeries, or other procedures. The symptoms of neurogenic bladder, especially incontinence, can severely degrade a person's quality of life.

The urethral sphincters are two muscles used to control the exit of urine in the urinary bladder through the urethra. The two muscles are either the male or female external urethral sphincter and the internal urethral sphincter. When either of these muscles contracts, the urethra is sealed shut.
A urethrocele is the prolapse of the female urethra into the vagina. Weakening of the tissues that hold the urethra in place may cause it to protrude into the vagina. Urethroceles often occur with cystoceles. In this case, the term used is cystourethrocele.
Urogynecology or urogynaecology is a surgical sub-specialty of urology and gynecology.

Urodynamic testing or urodynamics is a study that assesses how the bladder and urethra are performing their job of storing and releasing urine. Urodynamic tests can help explain symptoms such as:
Overflow incontinence is a concept of urinary incontinence, characterized by the involuntary release of urine from an overfull urinary bladder, often in the absence of any urge to urinate. This condition occurs in people who have a blockage of the bladder outlet, or when the muscle that expels urine from the bladder is too weak to empty the bladder normally. Overflow incontinence may also be a side effect of certain medications.

An artificial urinary sphincter (AUS) is an implanted device to treat moderate to severe stress urinary incontinence, most commonly in men. The AUS is designed to supplement the function of the natural urinary sphincter that restricts urine flow out of the bladder.
A urethral diverticulum is a condition where the urethra or the periurethral glands push into the connective tissue layers (fascia) that surround it.
Urethral hypermobility is a condition of excessive movement of the female urethra due to a weakened urogenital diaphragm. It describes the instability of the urethra in relation to the pelvic floor muscles. A weakened pelvic floor muscle fails to adequately close the urethra and hence can cause stress urinary incontinence. This condition may be diagnosed by primary care providers or urologists. Treatment may include pelvic floor muscle exercises, surgery, or minimally invasive procedures.

If medical treatment is not effective, surgery may need to be performed for benign prostatic hyperplasia.
These procedures aim to inject bio-compatible material into the walls of the anal canal, in order to bulk out these tissues. This may bring the walls of the anal canal into tighter contact, raising the resting pressure, creating more of a barrier to the loss of stool, and thereby reducing fecal incontinence. This procedure has many advantages over more invasive surgery, since there are rarely any serious complications.
References
- Hoffman, Barbara (2012). Williams gynecology, 2nd edition. New York: McGraw-Hill Medical. pp. 1198–1199. ISBN 0071716726. 1 2 3 4 5 Walters, Mark (2015). Urogynecology and reconstructive pelvic surgery, Chapter 22. Philadelphia, PA: Elsevier/Saunders. ISBN 9780323113779; Access provided by the University of Pittsburgh
- ↑ Hoffman, Barbara (2012). Williams gynecology, 2nd edition. New York: McGraw-Hill Medical. pp. 1198–1199. ISBN 978-0071716727.
- 1 2 3 4 5 Walters, Mark (2015). Urogynecology and reconstructive pelvic surgery, Chapter 22. Philadelphia, PA: Elsevier/Saunders. ISBN 9780323113779; Access provided by the University of Pittsburgh
{{cite book}}: CS1 maint: postscript (link)