Staging modalities
CT and PET scans
The mainstay of non-invasive staging is a CT scan of the chest followed by metabolic imaging with a PET scan. The CT scan shows abnormalities such as a lung nodule or enlarged lymph nodes whereas the PET scan reveals increased metabolism such as occurs in structures which contain rapidly growing cancer cells. PET/CT combined the benefits of functional assessment with PET and anatomic assessment with CT. PET/CT represents a significant advance for staging of patients with lung cancer with management impact in the order of 40% [25] and discordant findings compared with conventional imaging in half of patients. [25] PET/CT also has high inter- and intra-reporter agreement. [26] The main benefit of PET is to identify distant metastatic disease, thereby indicating futility of locoregional approaches such as surgery or curative intent radiotherapy.
According to the American College of Chest Physicians (ACCP) Non-Invasive Staging Guidelines for Lung Cancer (2007), [27] the pooled sensitivity and specificity of CT scanning for identifying mediastinal lymph node metastasis are 51% and 85%, respectively and for PET scanning 74% (95% CI, 69 to 79%) and 85% (95% CI, 82 to 88%), respectively. In other words, were one to rely on the results of non-invasive staging alone, between 21 and 31 percent of patients would be understaged (the cancer is more advanced than it seems) and between 12 and 18 percent of patients would be overstaged ( the cancer is in fact in an earlier stage than it seems). In selected clinical situations confirmation of the results of the status of the mediastinal nodes by sampling will therefore be necessary. [28]
PFTs
Pulmonary function tests (PFT) are not a formal part of staging but can be useful in treatment decisions. Patients with lung cancer resulting from air pollution (occupational or cigarette smoking-related) are more likely to have other lung disorders such as COPD, which limit their respiratory reserve. Patients with limited respiratory reserve are at higher risk for postoperative complications should surgical treatment be pursued; they may not be able to tolerate the diminished lung capacity remaining after the removal of a portion of the lung.
Brain MRI
PET scans need to be specifically modulated to detect metastases within the brain, which otherwise shows fairly uniformly active uptake from normal brain activity. In practice, CT or MRI scans are used to detect brain metastases. [10] Although MRI has a modestly higher detection rate [10] and can find smaller metastases, [10] contrast-enhanced CT scan can be a suitable choice [10] due to many factors such as MRI-incompatible metal prosthetics, claustrophobia, or noise-intolerance.
Mediastinal staging
Nearly half of lung cancers have mediastinal disease at diagnosis. [29] If cancer involves any of the mediastinal lymph nodes, these lymph nodes are designated N2 if they are on the same side as the original tumor, and N3 if they are on the other. N2, and particularly N3 lymph nodes, affect the clinical stage very significantly. The American Thoracic Society has standardized the nomenclature of lymph nodes in the chest. [30] There are fourteen numbered nodal stations. Lymph nodes considered to be in the mediastinum are stations 1–9, which are thus potential N2 or N3 locations, while stations 10-14 are hilar and peripheral nodes, and thus potential N1 locations.
There are numerous modalities which allow staging of mediastinal lymph nodes. In the following table they are arranged from the most to the least invasive.
| Procedure | Advantages | Disadvantages |
|---|---|---|
| Thoracotomy (surgical opening of the chest) | Allows the most thorough inspection and sampling of lymph node stations, may be followed by resection of tumor, if feasible | Most invasive approach, not indicated for staging alone, significant risk of procedure-related morbidity |
| Extended cervical mediastinoscopy combined with a Chamberlain procedure, which is also called a left parasternal mediastinotomy, or anterior mediastinotomy | Permits evaluation of the lymph nodes of the aortopulmonary space | More invasive; false-negative rate approximately 10%. |
| Chamberlain procedure | Access to station 5 (lymph nodes of the aortopulmonary space) | Limited applications, invasive. |
| Cervical mediastinoscopy | Still considered the gold standard (usual comparitor) by many, excellent for 2RL 4RL. | Does not cover all medastinal lymph node stations, particularly subcarinal lymph nodes (station 7), paraesophageal and pulmonary ligament lymph nodes (stations 8 and 9), the aortopulmonary space lymph nodes (station 5), and the anterior mediastinal lymph nodes (station 6); false-negative rate approximately 20%; invasive |
| Video-assisted thoracoscopy | Good for inferior mediastinum, station 5 and 6 lymph nodes | Invasive, does not cover superior anterior mediastinum |
| Transthoracic percutaneous fine needle aspiration (FNA) under CT guidance | More widely available than some other methods | Traverses a lot of lung tissue, therefore high pneumothorax risk, some lymph node stations inaccessible |
| Bronchoscopy with blind transbronchial FNA (Wang needle) | Less invasive than above methods | Relatively low yield, not widely practiced, bleeding risk |
| Endobronchial ultrasound (EBUS) | Direct visualization of lymph node stations. Complements EUS: covers lymph node stations 2R and 4R which are difficult to access by EUS; lower false-negative rate than with blind transbronchial FNA and fewer complications | More invasive than EUS, few practitioners, but rapidly growing in popularity |
| Endoscopic ultrasound (EUS) | Least invasive modality, uses the esophagus to access mediastinal lymph nodes, excellent for station 5, 7, 8 lymph nodes. Useful for station 2L and 4L, L adrenal, celiac lymph node | Cannot reliably access right sided paratracheal lymph node stations 2 R and 4R; accurate discrimination of primary hilar tumors and involved lymph nodes is important |
Endoscopic ultrasound



Background
This section focuses on the emerging role various types of endoscopic ultrasound and biopsy are playing in the diagnosis and staging of lung cancer, with an emphasis on the most common type of lung cancer, non-small cell lung cancer (NSCLC). These techniques have been reviewed extensively [29] [31] and have attained substantial consensus in guidelines such as from the NCCN.[ citation needed ]
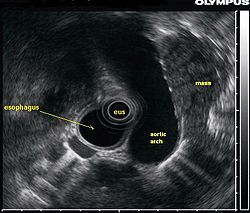
Endoscopic ultrasound (EUS) is an endoscopic technique where a miniaturized ultrasound probe is passed through the mouth into the upper gastrointestinal tract to investigate organs and structures close to the esophagus, stomach, or duodenum, such as the lung. In 1993, Wiersema published the first description of EUS to diagnose and stage lung cancer, [32] done by advancing a fine needle through the esophagus into adjacent lymph nodes. Numerous subsequent studies have shown this general methodology to be effective, very safe, minimally invasive, and very well tolerated. Given these advantages, many authorities think that EUS together with endobronchial ultrasound (EBUS) enhances lung cancer diagnosis and staging. [33]
Endoscopic ultrasound (EUS)
A metaanalysis published in 2007, based on 1,201 cancers in 18 high-quality clinical trials carefully selected by predefined criteria from the literature, systematically examined the performance of EUS-guided FNA in NSCLC staging. Two scenarios were considered: the setting of enlarged lymph nodes on CT (suggestive but not diagnostic of cancer), and the obverse scenario of an absence of lymph node enlargement on CT (suggestive but not diagnostic of no cancer). [29] Overall, in both settings, minor complications were reported in 0.8% of procedures; no major complications were recorded. EUS-FNA in enlarged discrete mediastinal lymph nodes had an excellent pooled sensitivity (8 studies) of 90% (95% CI, 84 to 94%) and specificity of 97% (95% CI, 95 to 98%).[ citation needed ] EUS-FNA in the setting of no enlarged mediastinal lymph nodes on CT had a pooled sensitivity (4 studies) of 58% (95% CI, 39 to 75%) and specificity of 98% (95% CI, 96 to 99%).[ citation needed ] Although this sensitivity (58% in CT-negative disease) might on first consideration seem disappointing, if EUS is performed as a staging test it can help avoid more invasive staging procedures, or surgery, if positive (for the presence of cancer). In other words, an EUS that has a positive result (shows cancer) will avoid further needless surgery, whereas a result not showing cancer may be false-negative, and probably requires an excisional biopsy technique for confirmation, such as VATS or mediastinoscopy.[ citation needed ]
The ACCP guidelines recommend invasive staging for patients with or without mediastinal lymph node enlargement on CT regardless of the PET scan findings.[ citation needed ] If needle techniques are used (such as EUS-NA, TBNA, EBUS-NA, or TTNA) a non-malignant result should be further confirmed by mediastinoscopy as explained above.[ citation needed ]
EUS can reliably reach the lymph node stations 5, 7, 8 and 9. In the superior mediastinum the trachea is somewhat to the right of the esophagus which makes it often possible to reach left-sided area 2 and 4 lymph nodes and, less often, right sided paratracheal lymph nodes. [34] In general, EUS is most appropriate for evaluation of the posterior inferior mediastinum while mediastinoscopy or EBUS are best for the anterior superior mediastinum. The feasibility of EUS-FNA of aorto-pulmonary space (subaortic) lymph nodes (station 5) is a major advantage of EUS. Evaluation of this station has traditionally required a paramedian mediastinotomy (Chamberlain procedure). EUS can easily sample celiac lymph nodes, which cannot be reached by the other mediastinal staging methods. In one recent study an unexpectedly high incidence of celiac lymph node metastasis (11%) was noted. [35] EUS can also be used to biopsy potential left adrenal metastases, whereas the right adrenal gland is mostly inaccessible. [36]
The potential utility of EUS-FNA in restaging of the mediastinum in patients who have undergone chemotherapy and radiotherapy for N2 or N3 disease is under investigation. The underlying idea is that initially advanced cancers, previously too extensive for surgery, may have responded to chemotherapy and radiation so much that they now may be operative candidates. Rather than immediately proceeding to thoracotomy based on CT or PET results, which could lead to an "open and close" thorax surgery, restaging, including invasive staging, may deselect non-responders, missed on imaging tests alone. If the initial mediastinal staging included a mediastinoscopy, most surgeons try to avoid a repeat mediastinoscopy after radiation treatment because of scarring. Although restaging by PET and CT scanning may help to provide targets for biopsies, the concept is that even PET-negative mediastinums need to be sampled. In N2 disease, EUS-FNA and EBUS-FNA appear to offer the best risk-benefit ratio in these patients. [37]
Endobronchial ultrasound (EBUS)
As mentioned in the table, EUS cannot reliably access right sided paratracheal lymph node stations 2R and 4R and may not be optimal for the left sided paratracheal lymph node stations either. An adaptation of the endoscopic ultrasound scope originally designed for the gastrointestinal tract is known as endobronchial ultrasound (EBUS). The instrument is inserted into the trachea rather than the esophagus. There are two types of EBUS bronchoscopes available: radial catheter probe and convex probe EBUS (CP-EBUS), [38] but only the latter concerns us here. Early experience with mediastinal staging by CP-EBUS appears very promising with sensitivities ranging from 92 to 96 percent in 4 series comprising 70 to 502 patients. [39] [40] [41] [42]
Combined ultrasound
Many patients will, if given a choice, prefer an instrument which is inserted into the esophagus (EUS) over one which is inserted into the trachea (EBUS). Furthermore, many patients with suspected lung cancer will have other smoking related illnesses, such as emphysema or COPD, which makes a bronchoscopy-like procedure (EBUS) a higher risk than an upper endoscopy through the esophagus (EUS). An area of active and emerging research concerns the value of combining EUS and EBUS in a single session, one specialist following the other, or -even more convenient- a dual trained operator doing one or the other – or both- as needed.
EUS-FNA and EBUS-FNA are complementary techniques. EUS has the highest yield in the posterior inferior mediastinum, and EBUS is strongest for the superior anterior mediastinum. Some lymph node stations can only be accessed by one method and not the other (for example, station 2 and 4 L and 3 are hard or impossible to see by EUS, stations 5 and 8 cannot be biopsied by EBUS). Together, EBUS and EUS cover the entire mediastinum (except possibly station 6) and complete mediastinal staging should be possible with a combination of these two procedures. This combination could conceptually eliminate the need for most surgical mediastinoscopies and in fact be more comprehensive.
When combined, this approach has been termed "complete medical mediastinoscopy." EUS-FNA with EBUS may allow near-complete, minimally invasive mediastinal staging in patients with suspected lung cancer [43]