In the English language, medical terms generally have a regular morphology, often being compound words that comprise three kinds of morphemes:[citation needed]roots, prefixes, and suffixes.[1][2] The etymology of medical terms often originates from Latin (particularly Neo-Latin)[3][4] and Ancient Greek,[5] with such medical terms being examples of neoclassical compounds. Each language may supply relevant morphemes for medical terms. For example, there are two primary roots for medical terminology relating to kidneys – one from Greek (νεφρός nephr(os)) and one from Latin (ren(es)).[citation needed]
The word root is developed to include a vowel sound following the term to add a smoothing action to the sound of the word when applying a suffix. The result is the formation of a new term with a vowel attached (word root + vowel) called a combining form. In English, the most common vowel used in the formation of the combining form is the letter -o-, added to the word root. For example, if there is an inflammation of the stomach and intestines, this would be written as gastro- and enter- plus -itis, gastroenteritis.[citation needed]
The formation of plurals should usually be done using the rules of the source language. Greek and Latin each have differing rules to be applied when forming the plural form of the word root.[citation needed]
Affixes
Prefixes and suffixes, primarily in Greek—but also in Latin, have a droppable -o-. As a general rule, this vowel almost always acts as a joint-stem to connect two consonantal roots (e.g. arthr- + -o- + -logy = arthrology), but generally, the -o- is dropped when connecting to a vowel-stem (e.g. arthr- + -itis = arthritis, instead of arthr-o-itis). Generally, Greek prefixes go with Greek suffixes and Latin prefixes with Latin suffixes. Although it is technically considered acceptable to create hybrid words, it is strongly preferred in coining new terms not to mix different lingual roots. Examples of accepted medical words that do mix lingual roots are neonatology and quadriplegia.[citation needed]
Prefixes do not normally require further modification to be added to a word root because the prefix normally ends in a vowel or vowel sound, although in some cases they may assimilate slightly and an in- may change to im- or syn- to sym-.[citation needed] Suffixes are attached to the end of a word root to add meaning such as condition, disease process, or procedure.[citation needed] Suffixes are categorized as either (1) needing the combining form, or (2) not needing the combining form since they start with a vowel.[citation needed]
Descriptive human anatomy often uses terminology that is fairly correct descriptive Latin. For example, musculus gluteus maximus simply means the "largest rump muscle", where musculus was Latin for "little mouse" and applied to muscles;[13] a frenum, a structure for keeping something in place, is Latin for bridle; and a foramen is Latin for a passage or perforation.[14]
A standardised set of terminology is used in anatomy to describe relative and absolute location and movement of anatomical parts.[15] The standard anatomical position is the orientation that anatomical terms of location and motion are typically used in reference to.[15] In humans, this refers to the body in a standing position with arms at the side and palms facing forward.[15] Other positions referenced in medicine include prone (lying facing down) and supine (lying facing up).[16]
Planes and axes
The three anatomical planes of the body: the sagittal, transverse (or horizontal), frontal planes
Relative to the standard anatomical position, three anatomical planes are widely used in medicine:
The three main axes of a human are the left-right (or horizontal or frontal), the craniocaudal (or rostrocaudal, longitudinal, or cephalocaudal),[a] and the anteroposterior (or dorsoventral or sagittal) axes.[24][25][26][b] Other anatomical lines include the axillary lines, parasternal line, and scapular line.
Many anatomical terms can be combined to indicate a position in two axes simultaneously or the direction of a movement relative to the body: Anterolateral indicates a position that is both anterior and lateral to the standard anatomical position (such as the bulk of the pectoralis major muscle) or a named organ such as the anterolateral tibial tubercle;[36][37] anteromedial is used, for example, in the anteromedial central arteries;[38] proximodistal describes the axis of an appendage such as an arm or a leg, taken from its tip at the distal part to where it joins the body at the proximal part.[39] Combined terms were once generally hyphenated, but typically the hyphen is omitted.[40]
In radiology, various X-ray views use terminology based on where the X-ray beam enters and leaves the body, including the front to back view (anteroposterior), the back to front view (posteroanterior), and the side view (lateral).[41]
The human body is shown in anatomical position in an anterior view and a posterior view. The regions of the body are labeled in boldface.The anatomical position, with terms of relative location noted
Motion
Terms of general motion
Terms
Movement
Definition
Etymology
Related terms
Ref
Abduction and adduction
Abduction
Pulls a structure away from a sagittal plane, carried out by one or more abductor muscles.
Circumduction is a conical movement of a body part, such as a ball and socket joint or the eye. Circumduction is a combination of flexion, extension, adduction and abduction. Circumduction may be performed at ball and socket joints, such as the hip and shoulder, as well as other parts of the body such as fingers, hands, feet, and head.[53] For example, circumduction occurs when spinning the arm when performing a serve in tennis or bowling a cricket ball.[54]
Flexion of the wrist joint, towards the palm and ventral side of forearm. (In anatomical position, the front and back of the arm are, respectively, considered ventral and dorsal.)
Flexion in the direction of the back of the foot. (The direction of terms are opposite to those in the hand because of embryological rotation of the limbs in opposite directions.)
The integumentary system is the set of organs forming the outermost layer of the human body, comprising the skin, hair, and nails. It acts as a protective physical barrier between the external environment and the internal environment, while maintaining water balance, protecting deeper tissue, excreting waste, and regulating body temperature.[66]
The skin (or, integument) is a composite organ, made up of the outermost epidermis and the inner dermis.[67] The epidermis comprises five layers: the stratum corneum, stratum granulosum, stratum spinosum and stratum basale. Where the skin is thicker, such as in the palms and soles, there is an extra layer of skin between the stratum corneum and the stratum granulosum known as the stratum lucidum. The dermis comprises two sections, the papillary and reticular layers, and contains connective tissues, blood vessels, glands, follicles, hair roots, sensory nerve endings, and muscular tissue.[68] Between the integument and the deep body musculature there is a transitional subcutaneous zone, the hypodermis.[69]
Bones are surrounded by a membrane known as the periosteum (Greek περῐ́ (perí), around; Greek ὀστέον (ostéon), bone), and comprise multiple layers, depending on the type of bone, including yellow and red bone marrow, spongy bone, and the endosteum. There are five general classifications of bones:
Long bones are characterized by a shaft known as the diaphysis, which is much longer than its width, and an epiphysis (Greek ἐπι- (epi-) upon, outside, over), a rounded head at each end of the shaft, connected to the diaphysis by the epiphyseal plate. They are made up mostly of compact bone, with lesser amounts of marrow, located within the medullary cavity, and areas of spongy, cancellous bone at the ends of the bones.[71]
Short bones are roughly cube-shaped, and have only a thin layer of compact bone surrounding a spongy interior. Short bones provide stability and support as well as some limited motion.[72]
Flat bones are thin and generally curved, with two parallel layers of compact bone sandwiching a layer of spongy bone.[73]
Sesamoid bones are bones embedded in tendons. Since they act to hold the tendon further away from the joint, the angle of the tendon is increased and thus the leverage of the muscle is increased.[74]
Irregular bones do not fit into the above categories. They consist of thin layers of compact bone surrounding a spongy interior. As implied by the name, their shapes are irregular and complicated. Often this irregular shape is due to their many centers of ossification or because they contain bony sinuses.[75]
A tendon is a tough, flexible band of fibrous connective tissue that connects muscles to bones. The extra-cellular connective tissue between muscle fibers binds to tendons at the distal and proximal ends, and the tendon binds to the periosteum of individual bones at the muscle's origin and insertion. As muscles contract, tendons transmit the forces to the relatively rigid bones, pulling on them and causing movement. Tendons can stretch substantially, allowing them to function as springs during movement.
Joints, also known as articulations, are structures that connect individual bones and may allow bones to move against each other to cause movement. Joints can be classified by structure and by function. Structurally, synovial joints are joints that are not directly joined, which are lubricated by a solution called synovial fluid;[77]fibrous, bony, and cartilaginous joints are characterised by the presence of their respective connective tissues. There are three functional divisions of joints:
Diarthroses, which allow extensive mobility between two or more articular heads.
False joints or synarthroses, which allow little or no movement and are predominantly fibrous.
A ligament is a small band of dense, white, fibrouselastic tissue.[78] Ligaments connect the ends of bones together in order to form a joint. Most ligaments limit dislocation, and prevent certain movements, such as hyperextension and hyperflexion, which may lead to breaks.[79]
An enthesis is the connective tissue that attaches tendons and ligaments to bones.[80]
The action of muscles often involve antagonistic pairs of agonist muscles and antagonist muscles, which, respectively, cause and inhibit a movement.[83]
Through the activation of agonist muscle, which produces most of the force and control of an action, movement occurs.[84]
Antagonist muscles are the muscles that produce an opposing joint torque to the agonist muscles.[85]
Synergist muscles, also called fixators or neutralisers, act around a joint to help, counter, or neutralise the action of an agonist muscle.[86]
Generally, as one muscle contracts, the other muscle relaxes in a process known as reciprocal inhibition.[87]Muscle contraction may be concentric (i.e. shortening), eccentric (i.e. lengthening), or isometric (i.e. involving no change in length).[88][89][90][91][92] Muscle groups (e.g. elbow flexors) are sometimes named based on the joint action they produce during concentric contraction.[93] During muscle contraction, the insertion of a muscle is the structure that is moved and is typically a bone that is distal and lighter than the origin; the origin is the bone, typically proximal, that remains more stable during contraction; the head of a muscle is the end part of the muscle that attaches to its origin.[94]
The circulatory system has two divisions, a systemic circuit (i.e. the left heart pumping oxygenated blood to the rest of the body (via the aorta) and into the right heart (via the venae cava)) and a pulmonary circuit (i.e. the right heart pumping deoxygenated blood to the lungs (via the pulmonary artery) and into the left heart (via the pulmonary vein)).[101][102][100] In the human heart:
Chambers of the heart are separated by the atrioventricular valves, which include the tricuspid valve on the right and the mitral valve on the left.[100]
The circulatory system processes an average of 20 litres of blood per day through capillary filtration, which removes plasma from the blood. Roughly 17 litres of the filtered blood are reabsorbed directly into the blood vessels. The lymphatic system provides an accessory return route to the blood for the remaining three litres of interstitial fluid.[104]
A lymph node is an organised collection of lymphoid tissue through which the lymph passes on its way back to the blood.[107] Lymph nodes are particularly numerous in the mediastinum, neck, pelvis, axilla, and inguinal region.[108]
Viscera are the internal organs of the ventral cavity.[117] The term "visceral" is contrasted with the term "parietal", meaning "of or relating to the wall of a body part, organ or cavity".[118] The two terms are often used in describing a membrane or piece of connective tissue, referring to the opposing sides.[119]
Contraction of the diaphragm (an upwardly domed sheet of muscle that separates the thoracic cavity from the abdominal cavity) and of the intercostal muscles (which lift up the ribs) increases the volume of the thoracic cavity.[121] Because of this increased volume, the lungs (which comprise elastic connective tissue) begin to inflate.[122][123][124]
Air, usually, enters from the nose.[125] From the nose, air travels into the trachea (the largest of airways) into the two main bronchi,[126] which branch into progressively narrower secondary and tertiary bronchi, which in turn branch into numerous smaller tubes known as the bronchioles,[126] which in turn open into the alveoli.[127]
Gallbladder: a hollow part of the biliary tract that sits just beneath the liver, with the gallbladder body resting in a small depression.[129] Commonly associated with gallstones, or cholelithiasis.[130]
The urinary system is the part of the excretory system that removes waste in the form of urine, comprising the kidneys, ureters, bladder, and the urethra. Other purposes of the urinary system include the regulation of blood volume and blood pressure; the control of electrolyte and metabolite levels; and the regulation of blood pH.[131] Each kidney consists of functional units called nephrons. Following filtration of blood and further processing, the ureters carry urine from the kidneys into the urinary bladder. During urination, the urethra carries urine out of the bladder through the penis or vulva. The female and male urinary system are very similar, differing only in the length of the urethra.[132]
Histology (also known as microanatomy or histoanatomy)[133][134][135] is the branch of medicine that studies the microscopic anatomy of biological tissues.[136][137][138][139] Histology is the microscopic counterpart to gross anatomy, which looks at larger structures visible without a microscope.[139][140]Histopathology is the branch of histology that includes the microscopic identification and study of diseased tissue.[141][142]
Smooth muscles control the flow of substances within the lumens of hollow organs, and are not consciously controlled. In the small intestine, smooth muscle contraction is characterised by peristalsis.
Skeletal muscles are attached to bones and arranged in opposing groups around joints. Skeletal muscles and cardiac muscles have striations, unlike smooth muscle. Only skeletal and smooth muscles are part of the musculoskeletal system and can move the body.[145]
Cardiac muscles are found in the heart and are used only to circulate blood; like the smooth muscles, these muscles are not under conscious control.
Connective tissue proper includes loose (or areolar) and dense (regular and irregular) connective tissue. Adipose (Latin adeps, adip-, fat) and reticular connective tissue are regarded by older sources as forms of loose connective tissue alongside areolar tissue, while some newer sources have termed them as forms of special connective tissue.[161]
Special connective tissue includes supportive connective tissue (bone and cartilage) and fluid connective tissue (blood and lymph).[162][163]
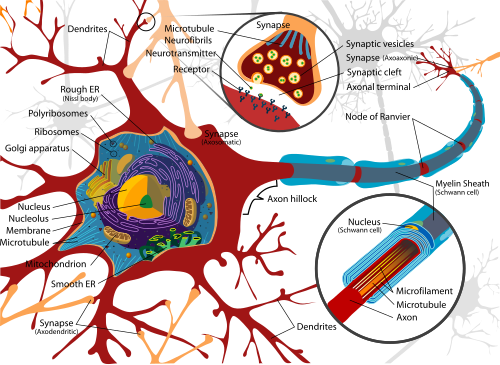
The neuron is the primary cell of the nervous system, supported structurally and metabolically by the glia.[170] Neurons comprise the following specialised organelles:
Dendrites, cellular extensions with many branches. The branches form fractal patterns that repeat at multiple size scales.[171] The majority of input to the neuron occurs via the dendritic spine.
Axon, a finer and longer cable-like projection. The axon primarily carries nerve signals away from the soma and carries some types of information back to it. Many neurons have only one axon, but this axon will usually undergo extensive branching, enabling communication with many target cells.
Axon terminal, found at the end of the axon farthest from the soma. Contains synapses.
Neurons communicate with other cells via synapses, specialised structures that connect neurons and facilitate the transmission of electrical and chemical signals.[172][173]
In electrical synapses, the presynaptic and postsynaptic cell membranes are connected by special channels called gap junctions that are capable of facilitating the direct flow of electrical current without the need for neurotransmitters, causing voltage changes in the presynaptic cell to induce voltage changes in the postsynaptic cell.[174][175][176]
In chemical synapses, the activation of voltage-gated calcium channels in the presynaptic neuron results in the release of neurotransmitters into the synaptic cleft, which thereafter bind to receptors located in the plasma membrane of the postsynaptic cell.
The neurotransmitter may initiate an electrical response or a secondary messenger pathway that may either excite or inhibit the postsynaptic neuron. Chemical synapses can be classified according to the neurotransmitter released: glutamatergic (often excitatory), GABAergic (often inhibitory), cholinergic (e.g. vertebrate neuromuscular junction), and adrenergic (releasing norepinephrine). Depending on their release location, the receptors they bind to, and the ionic circumstances they encounter, various transmitters can be either excitatory or inhibitory. For instance, acetylcholine can either excite or inhibit depending on the type of receptors it binds to.[177]
In excitatory synapses, an influx of Na+ driven by excitatory neurotransmitters opens cation channels, enhancing the probability of depolarization in postsynaptic neurons and the initiation of an action potential.
In inhibitory synapses, the opening of either Cl- or K+ channels diminish the probability of depolarization in postsynaptic neurons and the initiation of an action potential.
Astrocytes also exchange information with the synaptic neurons, responding to synaptic activity and, in turn, regulating neurotransmission.[172]
Summary showing different epithelial cells/tissues and their characteristics.
The basal surface of epithelial tissue rests on a basement membrane and the free, apical, or apex surface faces body fluid or the outside. The basement membrane acts as a scaffolding on which epithelium can grow and regenerate after injuries, and comprises the basal lamina and reticular lamina; although, some older sources use basement membrane and basal lamina synonymously.[178] The basement membrane acts as a selectively permeable membrane that determines which substances will be able to enter the epithelium, as epithelial tissue has a nerve supply though no blood supply.[179]:3
There are three principal shapes of epithelial cell: squamous (scaly), columnar, and cuboidal.[180]Transitional epithelium has cells that can change from squamous to cuboidal, depending on the amount of tension on the epithelium.[181] Epithelial tissue can be further categorised as having a singular layer of cells as simple epithelium; or as layers of two or more cells deep as stratified epithelium—stratified squamous epithelium, stratified cuboidal epithelium, and stratified columnar epithelium.[182]:94,97[183] When taller simple columnar epithelial cells are viewed in cross section showing several nuclei appearing at different heights, they can be confused with stratified epithelia, and are thus termed as pseudostratified columnar epithelium.[184] Epithelial cells are often ciliated.[185]
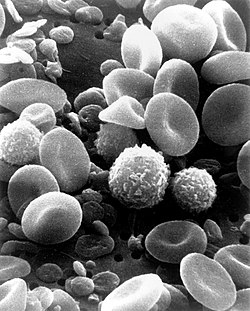
Leukocytes (commonly known as white blood cells) act like independent, single-celled organisms and are the second arm of the innate immune system. The innate leukocytes include:
The professional phagocytes, which generally patrol the body searching for pathogens, but can be called to specific locations by cytokines.[195] Once a pathogen has been engulfed by a phagocyte, it becomes trapped in an intracellular vesicle called a phagosome, which subsequently fuses with a lysosome vesicle to form a phagolysosome. The pathogen is then killed by the activity of digestive enzymes or following a respiratory burst that releases free radicals into the phagolysosome.[196][197]
Macrophages are cells that reside within tissues and produce an array of chemicals including enzymes, complement proteins, and cytokines. They also rid the body of worn-out cells and other debris and act as antigen-presenting cells that activate the adaptive immune system.[199]
Neutrophils are normally found in the bloodstream and are the most abundant type of phagocyte, representing 50% to 60% of total circulating leukocytes.[200] During the acute phase of inflammation, neutrophils migrate toward the site of inflammation in a process called chemotaxis and are usually the first cells to arrive at the scene of infection.
Dendritic cells are phagocytes in tissues that are in contact with the external environment, located mainly in the skin, nose, lungs, stomach, and intestines.[201] Dendritic cells are a link between bodily tissues and the innate and adaptive immune systems, as they present antigens to T cells.[201]
Basophils and eosinophils are related to neutrophils. They secrete chemical mediators that are involved in defending against parasites and play a role in allergic reactions, such as asthma.[205]
Natural killer cells (NK cells) do not directly attack invading microbes but destroy compromised host cells, such as tumor cells or virus-infected cells.[206][202] NK cells recognise such cells by a condition known as "missing self", which involves low levels of a cell-surface marker called MHC I (major histocompatibility complex)—a situation that can arise in viral infection.[207] Normal body cells are not recognized and attacked by NK cells because they express intact self MHC antigens, which inhibit NK cell activity.[208]
The major humoral component of the innate immune response is the complement system, a biochemical cascade that attacks the surfaces of foreign cells.[212][213] This response is activated by the binding of complement proteins to carbohydrates on the surfaces of microbes, or to antibodies that have attached to these microbes, which creates a cell signal that triggers a rapid killing response,[214] whose speed is significantly amplified after sequential proteolytic activation of complement protease molecules, controlled by positive feedback.[215] The cascade results in the production of peptides that attract immune cells; increase vascular permeability; and opsonize the surface of a pathogen, marking it for destruction. Complement binding can also kill cells directly by disrupting their plasma membrane via a membrane attack complex.[212]
Overview of the processes involved in the primary immune response
Inflammation
Inflammation is one of the first responses of the immune system to infection.[216] It is produced by eicosanoids and cytokines, which are released by injured or infected cells. In response to cytosolic PAMPs and DAMPs, pattern-recognition receptors called inflammasomes form in order to generate active forms of the inflammatory cytokines IL-1β and IL-18.[217]
Growth factors and cytotoxic factors may also be released. These chemicals recruit immune cells to the site of infection and promote the healing of any damaged tissue following the removal of pathogens.[221]
Adaptive immune system
The adaptive immune system allows for a stronger immune response as well as immunological memory, where each pathogen is "remembered" by a signature antigen.[222] The adaptive immune response is antigen-specific, allowing for the generation of tailored immune responses, and requiring the recognition of specific "non-self" antigens during a process called antigen presentation. The ability to mount these tailored responses is maintained in the body by memory T-cells and memory B-cells, which may be employed rapidly should a pathogen infect the body more than once.[223]
B cells and T cells are the major types of lymphocytes, which form the cells of the adaptive immune system.[224][225] B cells are involved in the humoral immune response, while T cells are involved in cell-mediated immune response. When B or T cells encounter their related antigens they multiply, and many "clones" of the cells are produced that target the same antigen. This is called clonal selection.[226] Some of the offspring of these B and T cells become long-lived memory cells, which remember each specific pathogen encountered and can mount a strong response if the pathogen is detected again. T-cells recognize pathogens by antigens that bind directly to T-cell surface receptors.[227] B-cells use the protein, immunoglobulin, to recognise pathogens by their antigens.[228]
Activation of macrophage or B cell by T helper cell
Killer T cells kill cells that are infected with pathogens or otherwise damaged or dysfunctional,[229] which contain a complex of a specific antigen coupled to a Class I MHC receptor. When the receptor of a cytotoxic or "killer" T-cell contacts such cells, it releases cytotoxins, such as perforin, which form pores in the target cell's plasma membrane, allowing ions, water and toxins to enter. The entry of another toxin called granulysin induces the target cell to undergo apoptosis.[230]
Helper T cells regulate both the innate and adaptive immune responses and help determine which immune responses the body makes to a particular pathogen.[231][232] These cells have no cytotoxic activity and do not kill infected cells or clear pathogens directly. They instead control the immune response by directing other cells to perform these tasks.[233]
A third, minor subtype are the γδ T cells, which recognise intact antigens that are not bound to MHC receptors.[234][235]
A B cell identifies pathogens when antibodies on its surface bind to a specific foreign antigen.[236] This antigen/antibody complex is taken up by the B cell and processed by proteolysis into peptides. The B cell then displays these antigenic peptides on its surface MHC class II molecules, which attracts a matching helper T cell that releases lymphokines and activates the B cell.[237] As the activated B cell then begins to divide, its offspring (plasma cells) secrete millions of copies of the antibody that recognizes this antigen. These antibodies circulate in blood plasma and lymph, bind to pathogens expressing the antigen and mark them for destruction by complement activation or for uptake and destruction by phagocytes. Antibodies can also neutralize challenges directly, by binding to bacterial toxins or by interfering with the receptors that viruses and bacteria use to infect cells.[238]
B cells and T cells are the major types of lymphocytes and are derived from hematopoietic stem cells in the bone marrow.[224] From the bone marrow, B cells immediately join the circulatory system and travel to secondary lymphoid organs in search of pathogens. T cells, on the other hand, travel from the bone marrow to the thymus, where they develop further, mature, and become immunocompetent. In the thymus, T cells are exposed to a wide variety of self-antigens;[245] T cells can only recognize a "non-self" target only after antigens have been processed and presented in combination with the major histocompatibility complex (MHC) self-receptor.[246] In contrast, the B cell antigen-specific receptor is an antibody molecule on the B cell surface, recognising unprocessed antigens (e.g. large molecules found on the surfaces of pathogens; small haptens, such as penicillin, attached to carrier molecules) without any need for antigen processing.[247] Each lineage of B cell expresses a different antibody, so the complete set of B cell antigen receptors represents all the antibodies that the human body can manufacture.[224]
Carcinoma: Cancers derived from epithelial cells. This group includes many of the most common cancers that occur in older adults. Nearly all cancers developing in the breast, prostate, lung, pancreas, and colon are carcinomas.
Lymphoma and leukemia: These two classes of cancer arise from immature cells that originate in the bone marrow, and are intended to fully differentiate and mature into normal components of the immune system and the blood, respectively. Acute lymphoblastic leukemia is the most common type of cancer in children, accounting for ~30% of cases.[251] However, far more adults than children develop lymphoma and leukemia.
Greek -ῖτις (-îtis) fem. form of -ίτης (-ítēs), pertaining to, because it was used with the feminine noun νόσος (nósos, disease), thus -îtis nósos, disease of the, disease pertaining to
Periods are generally not used.[261] Plurals for medical acronyms are represented by affixes a lowercase s with no apostrophe.[262] Arrows may also be used to indicate elevation (↑), diminution (↓), and causation (→, ←).[263]
Although some medical authorities recommend mirroring the terminology transgender people use to describe their own genitals, such usage may feel uncomfortable and intimate to some transgender people, who prefer to use different terms in medical contexts than they would in personal settings. At the same time, patients may also be uncomfortable with anatomical terms they perceive as gendered.[266]
Specialists recommend being open to using sex-neutral terms for organs, such as external genitals or lateral folds for the labia, internal reproductive organs for the uterus and ovaries, and chest for the breasts.[267]
The earliest known glossaries of medical terms were discovered on Egyptian papyrus authored around 1600 B.C.[270] Other precursors to modern medical dictionaries include lists of terms compiled from the Hippocratic Corpus in the first century AD.[271][272] The Synonyma Simonis Genuensis (the Synonyms of Simon of Genoa), attributed to the physician to Pope Nicholas IV in the year 1288, was printed by Antonius Zarotus at Milan in 1473. Referring to a copy held in the library of the College of Physicians of Philadelphia, Henry wrote in 1905 that "It is the first edition of the first medical dictionary."[273] However, this claim is disputed as the composition only included lists of herbs and drugs.[272]
At the beginning of the Renaissance, Italian universities began teaching a broader range of courses, such as law and medicine, whilst universities in northern Europe were still dominated by theology and related topics. All European universities required Latin proficiency for admission. Latin was the dominant language of university education, where rules were enforced against the use of vernacular languages.[274] Lectures and debates took place in Latin, and writing was in Latin, across the curriculum.
Latin dominated topics of international academic and scientific interest, especially at the level of abstract thought addressed to other specialists. To begin with, knowledge was already transmitted through Latin and it maintained specialised vocabularies not found in vernacular languages.[275] By the early modern period, Neo-Latin had become the lingua franca of science, medicine, legal discourse, theology, and education in Europe.[276] Over time, the use of Latin continued where international communication with specialist audiences was paramount. Later, where some of the discourse moved to French, English or German, translations into Latin would allow texts to cross language boundaries, while authors in countries with much smaller language populations or less known languages would tend to continue to compose in Latin.[277]
Latin's dominance over medicine began to change in the late seventeenth century, as philosophers and others began to write in their native language first, afterwards translating into Latin for international audiences.[278] In the early part of the 1700s, Latin was still making a significant contribution to academic publishing, but was no longer dominant.[279]
12Drake, Richard L.; Vogl, Wayne; Tibbitts, Adam W.M. Mitchell (2005). Gray's anatomy for students. illustrations by Richard Richardson, Paul (Pbk.ed.). Philadelphia: Elsevier/Churchill Livingstone. ISBN978-0-443-06612-2.
↑Dyce, Keith M.; Sack, Wolfgang O.; Wensing, Cornelis Johannes Gerardus (2010). Textbook of veterinary anatomy (4thed.). St. Louis, Mo: Saunders Elsevier. pp.2–3. ISBN978-1-4160-6607-1.
↑Moore, Keith L.; Dalley, Arthur F.; Agur, Anne M. R. (2018). Clinically oriented anatomy (Eighthed.). Philadelphia Baltimore New York London Buenos Aires Hong Kong Sydney Tokyo: Wolters Kluwer. pp.5–8. ISBN978-1-4963-4721-3.
↑Hyman, Libbie Henrietta (1979). Hyman's comparative vertebrate anatomy (3rded.). Chicago: Univ. of Chicago Pr. pp.1–6. ISBN978-0-226-87011-3.
↑Kardong, Kenneth V. (2019). Vertebrates: comparative anatomy, function, evolution (Eighth, international studented.). New York, NY: McGraw-Hill Education. p.16. ISBN978-1-260-09204-2.
↑"Introduction". Collection at Bartleby.com. 20 October 2022. Retrieved 1 March 2025.
↑Kardong, Kenneth V. (2019). Vertebrates: comparative anatomy, function, evolution (Eighth, international studented.). New York, NY: McGraw-Hill Education. p.16. ISBN978-1-260-09204-2.
↑Zhou, S; Zhao, Y; Sun, Z; Han, G; Xu, F; Qiu, W; Liu, T; Li, W (September 2024). "Impact of pelvic anteversion on spinopelvic alignment in an asymptomatic population: a dynamic perspective of standing and sitting". The Spine Journal. 24 (9): 1732–1739. doi:10.1016/j.spinee.2024.04.001. PMID38614156.
↑Moore, Keith L.; Dalley, Arthur F.; Agur, Anne M. R. (2018). Clinically oriented anatomy (Eighthed.). Philadelphia Baltimore New York London Buenos Aires Hong Kong Sydney Tokyo: Wolters Kluwer. p.679. ISBN978-1-4963-4721-3.
↑This article incorporates text available under the CC BY 4.0 license.Betts JG, Desaix P, Johnson E, Johnson JE, Korol O, Kruse D, Poe B, Wise J, Womble MD, Young KA (June 8, 2023). Anatomy & Physiology. Houston: OpenStax CNX. 6.2 Bone classification. ISBN978-1-947172-04-3.
↑Clarke B (2008), "Normal Bone Anatomy and Physiology", Clinical Journal of the American Society of Nephrology, 3 (Suppl 3): S131 –S139, doi:10.2215/CJN.04151206, PMC3152283, PMID18988698
↑Jerez A, Mangione S, Abdala V (2010), "Occurrence and distribution of sesamoid bones in squamates: a comparative approach", Acta Zoologica, 91 (3): 295–305, doi:10.1111/j.1463-6395.2009.00408.x, hdl:11336/74304
↑Bridwell, Keith. "Ligaments". Retrieved 16 March 2009.
↑Thomopoulos S, Birman V, Genin G, eds. (2012). Structural Interfaces and Attachments in Biology. New York: Springer. ISBN978-1-4614-3316-3.
↑Standring, Susan (2020). Gray's Anatomy: The Anatomical Basis of Clinical Practice (42nded.). New York. ISBN978-0-7020-7707-4. OCLC1201341621.{{cite book}}: CS1 maint: location missing publisher (link)
↑Widmaier, Eric P.; Raff, Hersel; Strang, Kevin T. (2010). "Muscle". Vander's Human Physiology: The Mechanisms of Body Function (12thed.). New York, NY: McGraw-Hill. pp.250–291. ISBN978-0-321-98122-6.
↑Baechle, Thomas (2008). Essentials of Strength Training and Conditioning. USA: National Strength and Conditioning Association. ISBN978-0-7360-8465-9.
↑Martini, Frederic; William C. Ober; Claire W. Garrison; Kathleen Welch; Ralph T. Hutchings (2001). Fundamentals of Anatomy and Physiology, 5th Ed. Prentice Hall. ISBN0-13-017292-8.
↑Hall, John E. (2011). Guyton and Hall textbook of medical physiology (Twelfthed.). Philadelphia, Pennsylvania. p.4. ISBN978-1-4160-4574-8.{{cite book}}: CS1 maint: location missing publisher (link)
↑Saladin, Kenneth S. (2011). Human anatomy (3rded.). New York: McGraw-Hill. p.520. ISBN978-0-07-122207-5.
↑Standring S (2016). Gray's anatomy: the anatomical basis of clinical practice (Forty-firsted.). Elsevier Limited. pp.68–73. ISBN978-0-7020-5230-9.
↑Standring, Susan (2016). Gray's anatomy: the anatomical basis of clinical practice (Forty-firsted.). [Philadelphia]: Elsevier Limited. p.1024. ISBN978-0-7020-5230-9.
12345Guyton, Arthur; Hall, John (2000). Guyton Textbook of Medical Physiology (10ed.). Saunders. ISBN978-0-7216-8677-6.
↑Saladin, Kenneth S. (2011). Human anatomy (3rded.). New York: McGraw-Hill. p.540. ISBN978-0-07-122207-5.
↑Pocock, Gillian; Richards, Christopher D. (2006). Human physiology: the basis of medicine (3rded.). Oxford: Oxford University Press. p.316. ISBN978-0-19-856878-0.
↑Levitzky, Michael G. (2013). Pulmonary physiology (Eighthed.). New York: McGraw-Hill Medical. p.Chapter 1. Function and Structure of the Respiratory System. ISBN978-0-07-179313-1.
12Gilroy, Anne M.; MacPherson, Brian R.; Ross, Lawrence M. (2008). Atlas of Anatomy. Stuttgart: Thieme. pp.108–111. ISBN978-1-60406-062-1.
↑Pocock, Gillian; Richards, Christopher D. (2006). Human physiology: the basis of medicine (3rded.). Oxford: Oxford University Press. pp.315–317. ISBN978-0-19-856878-0.
↑Hinic-Frlog, Sanja (2019). Introductory Animal Physiology. University of Toronto Mississauga: Pressbooks (CC BY 4.0). pp.40–59.
↑Drake RL, Vogl W, Mitchell AW, Richardson P (2005). Gray's Anatomy for students. Philadelphia: Elsevier/Churchill Livingstone. p.287. ISBN978-0-8089-2306-0.
↑Leeson, Thomas S.; Leeson, C. Roland (1981). Histology (Fourthed.). W. B. Saunders Company. p.600. ISBN978-0-7216-5704-2.
12Ross, Michael H.; Pawlina, Wojciech (2016). Histology: a text and atlas: with correlated cell and molecular biology (7thed.). Wolters Kluwer. pp.984p. ISBN978-1-4511-8742-7.
12Mooar, Pekka (2007). "Muscles". The Merck Manuals Online Medical Library. Retrieved 16 November 2008.
↑Baumann N, Pham-Dinh D (April 2001). "Biology of oligodendrocyte and myelin in the mammalian central nervous system". Physiological Reviews. 81 (2): 871–927. doi:10.1152/physrev.2001.81.2.871. PMID11274346.
↑Jessen KR, Mirsky R (September 2005). "The origin and development of glial cells in peripheral nerves". Nature Reviews. Neuroscience. 6 (9): 671–82. doi:10.1038/nrn1746. PMID16136171. S2CID7540462.
↑Young, Barbara; Lowe, James S.; Stevens, Alan; Heath, John W.; Deakin, Philip J. (2006). Wheater's Functional Histology: A Text and Colour Atlas (5thed.). Churchill Livingstone. ISBN978-0-443-06850-8.
↑Nelson, Fred R T; Blauvelt, Carolyn Taliaferro (2015). A Manual of Orthopedic Terminology (8thed.). Elsevier. p.70. ISBN978-0-323-22158-0.
↑Pawlina, Wojciech; Ross, Michael (2020). Histology: a text and atlas: with correlated cell and molecular biology (Eighthed.). Philadelphia: Wolters Kluwer Health. ISBN978-1-4963-8342-6.
12345Ross, Michael H.; Pawlina, Wojciech (2011). Histology: a text and atlas; with correlated cell and molecular biology (6., internationaled.). Philadelphia, Pa. London: Lippincott Williams & Wilkins. pp.158–173. ISBN978-0-7817-7200-6.
↑Moore, Keith; Dalley, Arthur (2005). Clinically Oriented Anatomy (5thed.). LWW. pp.47. ISBN0-7817-3639-0. A bundle of nerve fibers (axons) connecting neighboring or distant nuclei of the CNS is a tract.
↑J.H. Smith, C. Rowland, B. Harland, S. Moslehi, K. Schobert, R.M. Montgomery, W.J. Watterson, J. Dalrymple-Alford, R.P. Taylor, "How Neurons Exploit Fractal Geometry to Maximize Physical Connectivity", Scientific Reports, 11, 2332 (2021)
↑Jenkins GW, Tortora GJ (2013). Anatomy and Physiology from Science to Life (3rded.). John Wiley & Sons. pp.110–115. ISBN978-1-118-12920-3.
↑Ross MH, Pawlina W (2015). Histology: A Text and Atlas: With Correlated Cell and Molecular Biology (7thed.). Lippincott Williams & Wilkins. pp.528, 604. ISBN978-1-4511-8742-7.
↑Alberts B (2002). Molecular biology of the cell (4thed.). New York [u.a.]: Garland. p.1067. ISBN0-8153-4072-9.
↑Ryter A (1985). "Relationship between ultrastructure and specific functions of macrophages". Comparative Immunology, Microbiology and Infectious Diseases. 8 (2): 119–33. doi:10.1016/0147-9571(85)90039-6. PMID3910340.
↑Langermans JA, Hazenbos WL, van Furth R (Sep 1994). "Antimicrobial functions of mononuclear phagocytes". Journal of Immunological Methods. 174 (1–2): 185–94. doi:10.1016/0022-1759(94)90021-3. PMID8083520.
↑Kariyawasam HH, Robinson DS (Apr 2006). "The eosinophil: the cell and its weapons, the cytokines, its locations". Seminars in Respiratory and Critical Care Medicine. 27 (2): 117–27. doi:10.1055/s-2006-939514. PMID16612762. S2CID260317790.
↑Martin P, Leibovich SJ (Nov 2005). "Inflammatory cells during wound repair: the good, the bad and the ugly". Trends in Cell Biology. 15 (11): 599–607. doi:10.1016/j.tcb.2005.09.002. PMID16202600.
↑Harty JT, Tvinnereim AR, White DW (2000). "CD8+ T cell effector mechanisms in resistance to infection". Annual Review of Immunology. 18 (1): 275–308. doi:10.1146/annurev.immunol.18.1.275. PMID10837060.
↑McHeyzer-Williams LJ, Malherbe LP, McHeyzer-Williams MG (2006). "Helper T cell-regulated B cell immunity". From Innate Immunity to Immunological Memory. Current Topics in Microbiology and Immunology. Vol.311. pp.59–83. doi:10.1007/3-540-32636-7_3. ISBN978-3-540-32635-9. PMID17048705.
↑Holtmeier W, Kabelitz D (2005). "Γδ T Cells Link Innate and Adaptive Immune Responses". gammadelta T cells link innate and adaptive immune responses. Vol.86. pp.151–83. doi:10.1159/000086659. ISBN3-8055-7862-8. PMID15976493.{{cite book}}: |journal= ignored (help)
↑Sproul TW, Cheng PC, Dykstra ML, Pierce SK (2000). "A role for MHC class II antigen processing in B cell development". International Reviews of Immunology. 19 (2–3): 139–55. doi:10.3109/08830180009088502. PMID10763706. S2CID6550357.
↑Panksepp, J. (2003). Foreword to Cory, G. and Gardner, R. (2002) The Evolutionary Neuroethology of Paul MacLean: Convergences and Frontiers. ISBN978-0-275-97219-6[pageneeded]
↑Striedter, Georg F. (2005). "A History of Comparative Neurobiology". Principles of Brain Evolution. Sunderland, MA: Sinauer Associates. pp.19–50. ISBN978-0-87893-820-9. OCLC56532584. Reviewed in: Doty, Robert W. (June 2005). "Principles of Brain Evolution. By Georg F. Striedter. Sunderland (Massachusetts): Sinauer Associates. $59.95. xii + 436 p; ill.; index. ISBN 0-87893-820-6. 2005". The Quarterly Review of Biology. 80 (2): 264. doi:10.1086/433134. ISSN0033-5770.
↑Iverson, C.; Christiansen, S.; Flanagin, A.; etal. (2007). AMA Manual of Style (10thed.). Oxford University Press. ISBN978-0-19-517633-9.
↑Vera Pyle's Current Medical Terminology, 11th Ed., Health Professions Institute, Modesto, California, 2007, p. 174
↑The AAMT Book of Style for Medical Transcription, 2nd Ed., Peg Hughes, CMT, American Association for Medical Transcription, ISBN0-935229-38-8, copyright 2002
↑"Dosing: BID, TID". Global Antibiotic Research & Development Partnership. Depending on the drug class and its pharmacokinetic and pharmacodynamic properties, different dosing regimens may be optimal, including once a day (omne in die, OD), twice a day (bis in die, BID) or three times a day (ter in die, TID).
Edwards 2021, p.166. "An issue with mirrored language is that if people create names for their genitals, those names are much more likely to be names they use with intimate partners, not medical providers."
Hill-Meyer & Scarborough 2014, p.356. "For others, using clinical language is most comfortable because we feel it describes the body part that we have, not the gender we are.... Whatever we want to call our body parts is up to us. You might want to use different words in different contexts. Talking to medical providers and talking to lovers may call for different communication styles."
Ragosta et al. 2021, pp.712–713. "[F]ive TGE respondents noted that the term 'vagina' was either 'too clinical' or that they would only use 'vagina' in a medical context.... For 'period', [one] wrote, 'I use both; "period" to doctors that don't understand transgender, or use "shark week"'."
Bertok L, Chow D (2005). Bertok L, Chow D (eds.). Natural Immunity. Vol.5 (1sted.). Elsevier Science. ISBN978-0-44451-755-5.
Breinstrup, Thomas (2006). "Un revolution in le mundo scientific"[A revolution in the scientific world]. Historia de interlingua (in Interlingua). Archived from the original on 2019-04-27. Retrieved 2025-01-14.
Chung, Kyung Won (2005). Gross Anatomy (Board Review). Lippincott Williams & Wilkins. ISBN0-7817-5309-0.
Cook, Chad E. (2012). Orthopedic Manual Therapy: An Evidence Based Approach (2nded.). Upper Saddle River, NJ: Pearson Education. ISBN978-0-13-802173-3.
Breinstrup, Th.; Stenström, Ingvar; Olsson, Jesper, eds. (2007) [2001]. "Biographias: Ingvar Stenström". Interlingua (in Interlingua). Archived from the original on 2019-04-26. Retrieved 2025-01-15.
Dinour, Lauren M. (2019). "Speaking Out on 'Breastfeeding' Terminology: Recommendations for Gender-Inclusive Language in Research and Reporting". Breastfeeding Medicine. 14 (8). Mary Ann Liebert: 523–532. doi:10.1089/bfm.2019.0110. PMID31364867.
Fielding, Lucie (2021). Trans Sex: Clinical Approaches to Trans Sexualities and Erotic Embodiments. New York: Routledge. ISBN978-0-429-31829-0.
Gopsill, Frank Peter; Sexton, Brian (2006) [2001]. "Le natura, si – un schema, no". Historia de interlingua (in Interlingua). Archived from the original on 2022-04-12. Retrieved 2025-01-14.
Kendall, Florence Peterson; etal. (2005). Muscles: testing and function with posture and pain (5thed.). Baltimore, MD: Lippincott Williams & Wilkins. ISBN0-7817-4780-5.
Knight, Sarah; Tilg, Stefan, eds. (2015). The Oxford Handbook of Neo-Latin. New York: Oxford University Press. ISBN978-0-19-088699-8. OL28648475M.
McArthur, Tom (ed.): The Oxford Companion to the English Language, (Oxford University Press, 1992). ISBN0-19-214183-X
Murphy K, Weaver C (2016). Immunobiology (9ed.). Garland Science. ISBN978-0-8153-4505-3.
Plag, Ingo "Word-Formation in English", Cambridge University Press, 2003, ISBN à0521525632, 9780521525633
Rider, Nic G.; Caso, Taymy J.; Czech, Spencer; Karasic, Dan H. (2022). "Terminology in Transgender Medicine". In van Trotsenburg, Mick; Luikenaar, Rixt A. C.; Meriggiola, Maria Cristina (eds.). Context, Principles and Practice of TransGynecology: Managing Transgender Patients in ObGyn Practice. Cambridge UP. doi:10.1017/9781108899987. ISBN978-1-108-89998-7.
Stvrtinová V, Jakubovský J, Hulín I (1995). Pathophysiology: Principles of Disease. Computing Centre, Slovak Academy of Sciences: Academic Electronic Press.
Waquet, Françoise (2001). Latin, or the Empire of a Sign: From the Sixteenth to the Twentieth Centuries. Translated by John Howe. Verso. ISBN1859844022.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.