Health insurance or medical insurance is a type of insurance that covers the whole or a part of the risk of a person incurring medical expenses. As with other types of insurance, risk is shared among many individuals. By estimating the overall risk of health risk and health system expenses over the risk pool, an insurer can develop a routine finance structure, such as a monthly premium or payroll tax, to provide the money to pay for the health care benefits specified in the insurance agreement. The benefit is administered by a central organization, such as a government agency, private business, or not-for-profit entity.
The healthcare reform in China refers to the previous and ongoing healthcare system transition in modern China. China's government, specifically the National Health and Family Planning Commission, plays a leading role in these reforms. Reforms focus on establishing public medical insurance systems and enhancing public healthcare providers, the main component in China's healthcare system. In urban and rural areas, three government medical insurance systems—Urban Residents Basic Medical Insurance, Urban Employee Basic Medical Insurance, and the New Rural Co-operative Medical Scheme—cover almost everyone. Various public healthcare facilities, including county or city hospitals, community health centers, and township health centers, were founded to serve diverse needs. Current and future reforms are outlined in Healthy China 2030.
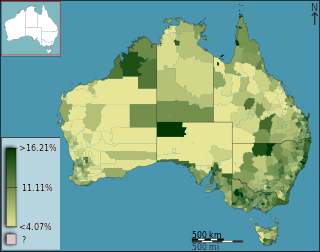
Health care in Australia operates under a shared public-private model underpinned by the Medicare system, the national single-payer funding model. State and territory governments operate public health facilities where eligible patients receive care free of charge. Primary health services, such as GP clinics, are privately owned in most situations, but attract Medicare rebates. Australian citizens, permanent residents, and some visitors and visa holders are eligible for health services under the Medicare system. Individuals are encouraged through tax surcharges to purchase health insurance to cover services offered in the private sector, and further fund health care.
Social security in India includes a variety of statutory insurances and social grant schemes bundled into a formerly complex and fragmented system run by the Indian government at the federal and the state level. The Directive Principles of State Policy, enshrined in Part IV of the Indian Constitution reflects that India is a welfare state. Food security to all Indians are guaranteed under the National Food Security Act, 2013 where the government provides highly subsidised food grains or a food security allowance to economically vulnerable people. The system has since been universalised with the passing of The Code on Social Security, 2020. These cover most of the Indian population with social protection in various situations in their lives.

Tanzania has a hierarchical health system which is in tandem with the political-administrative hierarchy. At the bottom, there are the dispensaries found in every village where the village leaders have a direct influence on its running. The health centers are found at ward level and the health center in charge is answerable to the ward leaders. At the district, there is a district hospital and at the regional level a regional referral hospital. The tertiary level is usually the zone hospitals and at a national level, there is the national hospital. There are also some specialized hospitals that do not fit directly into this hierarchy and therefore are directly linked to the ministry of health.

Employees' State Insurance Corporation is one of the two main statutory social security bodies under the ownership of Ministry of Labour and Employment, Government of India, the other being the Employees' Provident Fund Organisation. The fund is managed by the Employees' State Insurance Corporation (ESIC) according to rules and regulations stipulated in the ESI Act 1948.

Rashtriya Swasthya Bima Yojana is a government-run health insurance programme for the Indian poor. The scheme aims to provide health insurance coverage to the unrecognised sector workers belonging to the BPL category and their family members shall be beneficiaries under this scheme. It provides for cashless insurance for hospitalisation in public as well as private hospitals. The scheme started enrolling on April 1, 2008 and has been implemented in 25 states of India. A total of 36 million families have been enrolled as of February 2014. Initially, RSBY was a project under the Ministry of Labour and Employment. Now it has been transferred to Ministry of Health and Family Welfare from April 1, 2015

The National Health Mission (NHM) was launched by the government of India in 2005 subsuming the National Rural Health Mission and National Urban Health Mission. It was further extended in March 2018, to continue until March 2020. It is headed by Mission Director and monitored by National Level Monitors appointed by the Government of India.Rural Health Mission (NRHM) and the recently launched National Urban Health Mission (NUHM). Main program components include Health System Strengthening (RMNCH+A) in rural and urban areas- Reproductive-Maternal- Neonatal-Child and Adolescent Health, and Communicable and Non-Communicable Diseases. NHM envisages achievement of universal access to equitable, affordable and quality health care services that are accountable and responsive to the needs of the people.

Agriculture in India is highly susceptible to risks like droughts and floods. It is necessary to protect the farmers from natural calamities and ensure their credit eligibility for the next season. For this purpose, the Government of India introduced many agricultural social insurances throughout the country, the most important one of them being Pradhan Mantri Fasal Bima Yojana.
Achieving Universal Health Care has been a key goal of the Indian Government since the Constitution was drafted. The Government has since launched several programs and policies to realize ‘Health for All’ in the nation. These measures are in line with the sustainable development goals set by the United Nations. Health disparities generated through the Hindu caste system have been a major roadblock in realizing these goals. The Dalit (untouchables) community occupies the lowest stratum of the Hindu caste system. Historically, they have performed menial jobs like- manual scavenging, skinning animal hide, and sanitation. The Indian constitution officially recognizes the Dalit community as ‘Scheduled Castes’ and bans caste-based discrimination of any form. However, caste and its far-reaching effects are still prominent in several domains including healthcare. Dalits and Adivasis have the lowest healthcare utilization and outcome percentage. Their living conditions and occupations put them at high risk for disease exposure. This, clubbed with discrimination from healthcare workers and lack of awareness makes them the most disadvantaged groups in society.

India has a multi-payer universal health care model that is paid for by a combination of public and private health insurance funds along with the element of almost entirely tax-funded public hospitals. The public hospital system is essentially free for all Indian residents except for small, often symbolic co-payments in some services.

Mahatma Jyotiba Phule Jan Arogya Yojana, previously Rajiv Gandhi Jeevandayee Arogya Yojana (RGJAY), is a Universal health care scheme run by the Government of Maharashtra for the poor people of the state of Maharashtra who holds one of the 4 cards issued by the government; Antyodaya card, Annapurna card, yellow ration card or orange ration card. The scheme was first launched in 8 districts of the Maharashtra state in July 2012 and then across all 35 districts of the state in November 2015. It provides free access to medical care in government empanelled 488 hospitals for 971 types of diseases, surgeries and therapies costing up to Rs.1,50,000 per year per family. As of 17 January 2016, around 11.81 lakh procedures amounting to Rs.1827 crore have been performed on patients from 7.13 lakh beneficiary families which includes over 7.27 lakh surgeries and therapies. The scheme is called successful amid some allegations of hospitals directly or indirectly causing patients to incur out-of-pockets expenses on some part of the treatment.

Pradhan Mantri Ujjwala Yojana was launched by Prime Minister of India Narendra Modi on 1 May 2016 to distribute 50 million LPG connections to women of Below Poverty Line (BPL) families. A budgetary allocation of ₹80 billion (US$1.0 billion) was made for the scheme. The scheme was replaced by the Ujjwala Yojana 2.0 in 2021.

D Y Patil Hospital or D.Y.P.H.R.C. is a charitable hospital in Navi Mumbai, India. It was founded in 2004 by Shri Dnyandeo Yashwantrao Patil. It has 1500 beds dedicated to charity, a 300-bed ICU facility, 15 operation theatres, a 24x7 charitable casualty and trauma centre. It has a blood bank that is accredited by NABH. The hospital is one of the largest charitable hospitals in India.

Ayushman Bharat Pradhan Mantri Jan Arogya Yojana(PM-JAY) is a national public health insurance scheme of the Government of India that aims to provide free access to health insurance coverage for low income earners in the country. Roughly, the bottom 50% of the country qualifies for this scheme. People using the program access their own primary care services from a family doctor and when anyone needs additional care, PM-JAY provides free secondary health care for those needing specialist treatment and tertiary health care for those requiring hospitalization.
Biju Swasthya Kalyan Yojana is a universal health coverage scheme launched by Chief Minister of Odisha Naveen Patnaik. The scheme covers around 70 lakhs families. A budget of 250 crore was sanctioned by the state government. Cashless healthcare assistance will be provided. Services:
- Free health services for all in all state government health care facilities starting from Sub center level up to district headquarter hospital level with Swasthya Mitras deployed at help desk.
- Annual health coverage of Rs 5 lakhs per family and 7 lakhs per women members of the family.
The Twelfth Five Year plan for health services in India covering 2012-2017 was formulated based on the recommendation of a High Level Experts Group (HLEG) and other stakeholder consultations. The long-term objective of this strategy is to establish a system of Universal Health Coverage (UHC) in the country. Key points include:
- Substantial expansion and strengthening of public sector health care system, freeing the vulnerable population from dependence on high cost and often unreachable private sector health care system.
- Health sector expenditure by central government and state government, both plan and non-plan, will have to be substantially increased by the twelfth five-year plan. It was increased from 0.94 per cent of GDP in tenth plan to 1.04 per cent in eleventh plan. The provision of clean drinking water and sanitation as one of the principal factors in control of diseases is well established from the history of industrialized countries and it should have high priority in health related resource allocation. The expenditure on health should increased to 2.5 per cent of GDP by the end of Twelfth Five Year Plan.
- Financial and managerial system will be redesigned to ensure efficient utilization of available resources and achieve better health outcome. Coordinated delivery of services within and across sectors, delegation matched with accountability, fostering a spirit of innovation are some of the measures proposed.
- Increasing the cooperation between private and public sector health care providers to achieve health goals. This will include contracting in of services for gap filling, and various forms of effectively regulated and managed Public-Private Partnership, while also ensuring that there is no compromise in terms of standards of delivery and that the incentive structure does not undermine health care objectives.
- The present Rashtriya Swasthya Bima Yojana (RSBY) which provides cash less in-patient treatment through an insurance based system should be reformed to enable access to a continuum of comprehensive primary, secondary and tertiary care. In twelfth plan period entire Below Poverty Line (BPL) population will be covered through RSBY scheme. In planning health care structure for the future, it is desirable to move from a 'fee-for-service' mechanism, to address the issue of fragmentation of services that works to the detriment of preventive and primary care and also to reduce the scope of fraud and induced demand.
- In order to increase the availability of skilled human resources, a large expansion of medical schools, nursing colleges, and so on, is therefore necessary and public sector medical schools must play a major role in the process. Special effort will be made to expand medical education in states which are under-served. In addition, a massive effort will be made to recruit and train paramedical and community level health workers.
- The multiplicity of Central sector or Centrally Sponsored Schemes has constrained the flexibility of states to make need based plans or deploy their resources in the most efficient manner. The way forward is to focus on strengthening the pillars of the health system, so that it can prevent, detect and manage each of the unique challenges that different parts of the country face.
- A series of prescription drugs reforms, promotion of essential, generic medicine and making these universally available free of cost to all patients in public facilities as a part of the Essential Health Package will be a priority.
- Effective regulation in medical practice, public health, food and drugs is essential to safeguard people against risks and unethical practices. This is especially so given the information gaps in the health sector which make it difficult for individual to make reasoned choices.
- The health system in the Twelfth Plan will continue to have a mix of public and private service providers. The public sector health services need to be strengthened to deliver both public health related and clinical services. The public and private sectors also need to coordinate for the delivery of a continuum of care. A strong regulatory system would supervise the quality of services delivered. Standard treatment guidelines should form the basis of clinical care across public and private sectors, with the adequate monitoring by the regulatory bodies to improve the quality and control the cost of care,
Atal Bhujal Yojana is a groundwater management scheme launched by Prime Minister Narendra Modi on the 95th birth anniversary of former Prime Minister Atal Bihari Vajpayee, on 25 December 2019. The purpose of the scheme is to improve groundwater management in seven states of India.

Bharatiya Janata Party, Gujarat is the state unit of the Bharatiya Janata Party that operates in Gujarat. C. R. Patil currently serves as state president of the party. The leader of the party is Bhupendrabhai R Patel, the incumbent chief minister of Gujarat. The head office of the party is located in Gandhinagar, Gujarat.

