The signs and symptoms of frontal lobe disorder can be indicated by dysexecutive syndrome[7] which consists of a number of symptoms which tend to occur together.[8] Broadly speaking, these symptoms fall into three main categories; cognitive (movement and speech), emotional, or behavioral. Although many of these symptoms regularly co-occur, it is common to encounter patients who have several, but not all of these symptoms. This is one reason why some researchers are beginning to argue that dysexecutive syndrome is not the best term to describe these various symptoms. The fact that many of the dysexecutive syndrome symptoms can occur alone has led some researchers[9] to suggest that the symptoms should not be labelled as a "syndrome" as such. Some of the latest imaging research[10] on frontal cortex areas suggests that executive functions may be more discrete than was previously thought. Signs and symptoms can be divided as follows:[1]
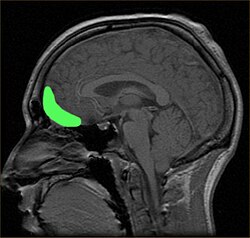
The causes of frontal lobe disorders can be closed head injury. An example of this can be from an accident, which can cause damage to the orbitofrontal cortex area of the brain.[2]
The frontal lobe contains the precentral gyrus and prefrontal cortex and, by some conventions, the orbitofrontal cortex. These three areas are represented in both the left and the right cerebral hemispheres. The precentral gyrus or primary motor cortex is concerned with the planning, initiation and control of fine motor movements dorsolateral to each hemisphere.[15] The dorsolateral part of the frontal lobe is concerned with planning, strategy formation, and other executive functions. The prefrontal cortex in the left hemisphere is involved with verbal memory while the prefrontal cortex in the right hemisphere is involved in spatial memory. The left frontal operculum region of the prefrontal cortex, or Broca's area, is responsible for expressive language, i.e. language production. The orbitofrontal cortex is concerned with response inhibition, impulse control, and social behaviour.[4]
The diagnosis of frontal lobe disorder can be divided into the following three categories:
Clinical history
Frontal lobe disorders may be recognized through a sudden and dramatic change in a person's personality, for example with loss of social awareness, disinhibition, emotional instability, irritability or impulsiveness. Alternatively, the disorder may become apparent because of mood changes such as depression, anxiety or apathy.[1]
A range of neuropsychological tests are available for clarifying the nature and extent of frontal lobe dysfunction. For example, concept formation and ability to shift mental sets can be measured with the Wisconsin Card Sorting Test, planning can be assessed with the Mazes subtest of the WISC.[3]Frontotemporal dementia shows up as atrophy of the frontal cortex on MRI.[20] Frontal impairment due to head injuries, tumours or cerebrovascular disease will also appear on brain imaging.[4]
Treatment
In terms of treatment for frontal lobe disorder, there is none, general supportive care is given, also some level of supervision could be needed. The prognosis will depend on the cause of the disorder, of course. A possible complication is that individuals with severe injuries may be disabled, such that, a caregiver may be unrecognizable to the person.[5] Another aspect of treatment of frontal lobe disorder is speech therapy. This type of therapy might help individuals with symptoms that are associated with aphasia and dysarthria.[4]
History
Phineas Gage, who sustained a severe frontal lobe injury in 1848, has been called a case of dysexecutive syndrome. Gage's psychological changes are almost always exaggerated–of the symptoms listed, the only ones Gage can be said to have exhibited are "anger and frustration", slight memory impairment, and "difficulty in planning".[21]
In December 2005, at his Dover Road flat in Singapore, 44-year-old caretaker Mohammad Zam Abdul Rashid attacked and battered his 38-year-old wife Ramona Johari (a production operator) to death after he accused her of getting close to a colleague. Mohammad Zam was originally charged with murder but after he was found to be suffering from frontal lobe syndrome, which went undiagnosed prior to the murder and had affected his mental responsibility at the time of the killing, Mohammad Zam was convicted of a reduced charge of manslaughter and hence sentenced to life imprisonment.[22] The diagnosis of frontal lobe syndrome in this homicide case generated public discussions about the disorder.[23]
↑Miller, Bruce L.; Cummings, Jeffrey L. (2007). The Human Frontal Lobes: Functions and Disorders. Guilford Publications. pp.19, 450. ISBN978-1-59385-329-7.
↑Niedermeyer, E (Jan 2001). "Frontal lobe disinhibition, Rett syndrome and attention deficit hyperactivity disorder". Clinical Electroencephalography. 32 (1): 20–3. doi:10.1177/155005940103200106. PMID11202137. S2CID35417045.
↑Leadership, Donald T. Stuss Reva James Leeds Chair in Neuroscience and Research; Berkeley, Helen Wills Neuroscience Institute Robert T. Knight Evan Rauch Professor of Neuroscience and Director, Department of Psychology University of California (20 June 2002). Principles of Frontal Lobe Function. Oxford University Press. p.13. ISBN978-0-19-803083-6.{{cite book}}: CS1 maint: multiple names: authors list (link)
↑Pangman, Verna C.; Sloan, Jeff; Guse, Lorna (2000). "An examination of psychometric properties of the Mini-Mental State Examination and the Standardized Mini-Mental State Examination: Implications for clinical practice". Applied Nursing Research. 13 (4): 209–13. doi:10.1053/apnr.2000.9231. PMID11078787.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.