Prevention involves avoidance of things which irritate the gut and which trigger symptoms, including alcohol, nonsteroidal anti-inflammatory drugs (NSAIDs), tobacco, and certain foods.[4][examples needed] It is also recommended to treat for any underlying H. pylori infection before starting NSAID treatment in order to prevent irritation and gastroduodenal ulcers.[7] Treatment includes medications such as antacids, H2 blockers, and proton pump inhibitors.[1] During an acute flare-up, drinking viscous lidocaine may help.[8] If gastritis is caused by NSAID use (e.g. aspirin, ibuprofen, naproxen), usage may be ceased.[1] If H. pylori is present, it may be treated with a combination of antibiotics such as amoxicillin and clarithromycin.[1] For those with pernicious anemia, vitamin B12 supplements are recommended by injection.[3]
Gastritis is believed to be present in 30% to 50% of people worldwide, but most cases are asymptomatic.[4] In 2013 there were approximately 90 million new cases of the condition.[9] The risk of developing gastritis increases as one ages.[4] Gastritis, along with a similar condition in the first part of the intestines called duodenitis, resulted in 50,000 deaths in 2015.[5]H. pylori was first discovered in 1981 by Barry Marshall and Robin Warren.[10]
Classification
Updated Sydney System (USS) for classification of gastritis based on morphological features.
There are multiple classification systems which may be used to categorise gastritis cases. The Updated Sydney System (USS) of 1994 is commonly used for classification, based primarily on the morphological features of the disease seen in endoscopic biopsies. The Kyoto system (from the 2015 Kyoto Consensus Conference) classifies gastritis based primarily on the cause and duration of symptoms, resulting in the 3 types acute, chronic, and special.[11] Gastritis may also be classified based on the kind of mucosal injury, resulting in the 2 types erosive and non-erosive.[12][13]
The Operative Link for Gastritis Assessment (OLGA) staging system may also be used to classify cases of gastritis.[14] The OLGA system was devised in an attempt to evaluate complication risk, in particular the development of gastritis into intestinal metaplasia or gastric cancer. The degree of atrophy and metaplasia at two main sites is scored on a four-tiered scale.[15]
Corpus
No atrophy (score 0)
Mild atrophy (score 1)
Moderate atrophy (score 2)
Severe atrophy (score 3)
Antrum (including incisura angularis)
No atrophy (score 0)
Stage 0
Stage I
Stage II
Stage II
Mild atrophy (score 1)
Stage I
Stage I
Stage II
Stage III
Moderate atrophy (score 2)
Stage II
Stage II
Stage III
Stage IV
Severe atrophy (score 3)
Stage III
Stage III
Stage IV
Stage IV
Signs and symptoms
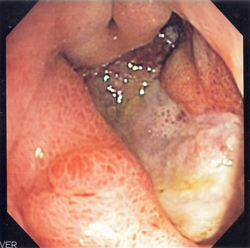
A peptic ulcer, which may accompany gastritis, seen via endoscopy.
Many people with gastritis experience no symptoms at all. However, upper central abdominal pain is the most common symptom; the pain may be dull, vague, burning, aching, gnawing, sore, or sharp.[16] Pain is usually located in the upper central portion of the abdomen, but it may occur anywhere from the upper left portion of the abdomen around to the back.[17]
Other signs and symptoms may include the following:[16]
Helicobacter pylori infection is the most common cause of gastritis; when contracted this way, it may be termed H. pylori gastritis.[18][19]H. pylori is a kind of bacteria which colonizes the gut of more than half of the world's population. While the bacteria is present in over half of the world's population, infection does not necessarily cause symptoms and thus most cases are asymptomatic.[20] It has been suggested that H. pylori plays an important role in the natural stomach ecology.[21]
Gastritis can result from usage of some drugs, the most common being usage of nonsteroidal anti-inflammatory drugs (NSAIDs) such as aspirin, ibuprofen, and naproxen. Other drugs include cocaine, iron, colchicine when administered at toxic levels, kayexalate (a kind of polystyrene sulfonate), ticlopidine, and those associated with chemotherapy and immunotherapy for cancer.[7][18] Drugs used for COVID-19 treatment have also been found to cause gastritis; tocilizumab and sarilumab are associated with chronic gastritis, while lopinavir/ritonavir is associated with the acute form.[7]
Gastritis is also associated with bile reflux, in which bile and/or pancreatic enzymes flow up into the stomach; when bile travels further upwards into the esophagus, it is called gastric reflux. Excessive refluxed bile in the stomach causes irritation and inflammation to the stomach lining, leading to the development of gastric ulcers and/or gastritis; when contracted this way, it may be termed bile reflux gastritis.[22][23]
Evidence does not support a role for specific foods, including spicy foods and coffee, in the development of peptic ulcers.[27] People are, however, usually advised to avoid foods that trigger symptoms.[28] There is little specific advice on diet published by authoritative sources. The National Health Service of the United Kingdom advises avoiding spicy, acidic or fried foods which may irritate the stomach.[29]
It is generally advised to avoid alcohol consumption for the prevention and mitigation of gastrointestinal injury.[4][7] Some sources describe alcohol as a potential cause of gastritis,[1][4][13] while others describe it instead as a potential contributor to the erosion of the stomach's mucosal lining when ingested in large doses.[30][31]
Diagnosis
Gastritis should be investigated when a patient reports abdominal discomfort, pain, and/or nausea.[13] Diagnosis relies primarily on the findings of an upper endoscopy with biopsy, but also involves taking a comprehensive patient history.[4][11] While history and other tests can help provide insights, histopathological examination of gastric biopsies are the gold standard, and allow one to identify the distribution, severity, and etiology of the disease.[11]
Other tests which may be ordered to diagnose or rule out gastritis include:
H. pylori testing by urea breath test, stool antigen test, endoscopic biopsy, or specific antibody test[4]
Antacids are a common treatment for mild to medium gastritis.[32] When antacids do not provide enough relief, medications such as H2 blockers and proton-pump inhibitors that help reduce the amount of acid are often prescribed.[32][33]
Cytoprotective agents are designed to help protect the tissues that line the stomach and small intestine.[34] They include the medications sucralfate and misoprostol. If NSAIDs are being taken regularly, one of these medications to protect the stomach may also be taken. Another cytoprotective agent is bismuth subsalicylate.[35]
Several regimens are used to treat H. pylori infection. Most use a combination of two antibiotics and a proton pump inhibitor. Sometimes bismuth is added to the regimen.[citation needed]
History
Gastric cancer was first described in 1000 A.D. by Persian physician Avicenna. In 1728, German physician Georg Ernst Stahl coined the term "gastritis". Italian anatomical pathologist Giovanni Battista Morgagni further described the characteristics of gastric inflammation, including the characteristics of erosive or ulcerative gastritis and erosive gastritis. Between 1808 and 1831, French physician François-Joseph-Victor Broussais gathered information from autopsies of dead French soldiers. He described chronic gastritis as "gastritide" and erroneously believed that gastritis was the cause of ascites, typhoid fever, and meningitis. In 1854, Charles Handfield Jones and Wilson Fox described the microscopic changes of the stomach's inner lining in gastritis. In 1855, Baron Carl von Rokitansky first described hypertrophic gastritis. In 1859, British physician William Brinton first described acute, subacute, and chronic gastritis. In 1870, Samuel Fenwick noted that pernicious anemia causes glandular atrophy in gastritis. German surgeon Georg Ernst Konjetzny noticed that both gastric ulcers and gastric cancer are the results of gastric inflammation. Shields Warren and Willam A. Meissner described the intestinal metaplasia of the stomach as a feature of chronic gastritis.[36]
Early acute superficial gastritis. Marked neutrophilic infiltrates appear in the mucous neck region and lamina with a pit microabscess. This case was caused by Helicobacter pylori.
Acute erosive gastritis typically involves discrete foci of surface necrosis due to damage to mucosal defenses.[37] NSAIDs inhibit cyclooxygenase-1, or COX-1, an enzyme responsible for the biosynthesis of eicosanoids in the stomach, increasing the likelihood of peptic ulcers forming.[38][39][40] NSAIDs also inhibit prostaglandin synthesis, a hormone with a protective effect on the stomach's mucosal lining. While short-term NSAID use causes no problems, long-term use can lead to gastritis or other complications.[41][30]
Metaplasia
Metaplasia is the transformation of differentiated cells from one type into another type. Mucous gland metaplasia can occur after severe damage to the gastric glands causes them to waste away (atrophic gastritis) and be progressively replaced by mucous glands. Gastric ulcers may develop; it is unclear if they are the causes or the consequences.[37]
Intestinal metaplasia typically begins in response to chronic mucosal injury in the antrum and may extend to the body. Gastric mucosa cells change to resemble intestinal mucosa and may even assume absorptive characteristics. Intestinal metaplasia is classified histologically as complete or incomplete. In the complete type, gastric mucosa is completely transformed into small-bowel mucosa, both histologically and functionally, with the ability to absorb nutrients and secrete peptides. In the incomplete type, the epithelium assumes a histologic appearance closer to that of the large intestine and frequently exhibits dysplasia.[37]
123456789101112131415161718"Gastritis". The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). November 27, 2013. Archived from the original on 6 March 2015. Retrieved 1 March 2015.
123Varbanova M, Frauenschläger K, Malfertheiner P (Dec 2014). "Chronic gastritis - an update". Best Pract Res Clin Gastroenterol. 28 (6): 1031–42. doi:10.1016/j.bpg.2014.10.005. PMID25439069.
↑Adams (2012). "32". Emergency Medicine: Clinical Essentials. Elsevier Health Sciences. ISBN978-1-4557-3394-1. Archived from the original on 2016-08-15.
↑Wang AY, Peura DA (October 2011). "The prevalence and incidence of Helicobacter pylori-associated peptic ulcer disease and upper gastrointestinal bleeding throughout the world". Gastrointestinal Endoscopy Clinics of North America. 21 (4): 613–635. doi:10.1016/j.giec.2011.07.011. ISSN1558-1950. PMID21944414.
1234Azer SA, Awosika AO, Akhondi H (2024-06-22), "Gastritis", StatPearls, StatPearls Publishing, PMID31334970, retrieved 2025-11-27
↑"Gastritis". National Digestive Diseases Information Clearinghouse. National Institute of Diabetes and Digestive and Kidney Diseases. December 2004. Archived from the original on 2008-10-11. Retrieved 2008-10-06.
12Siegelbaum J (23 August 2019). "GI Health Resources > Gastritis". Jackson Siegelbaum Gastroenterology. Archived from the original on 15 June 2021. Retrieved 25 February 2022.
12Zajac P, Holbrook A, Super ME, Vogt M (March–April 2013). "An overview: Current clinical guidelines for the evaluation, diagnosis, treatment, and management of dyspepsia". Osteopathic Family Physician. 5 (2): 79–85. doi:10.1016/j.osfp.2012.10.005.
↑Fashner J, Gitu AC (15 February 2015). "Diagnosis and Treatment of Peptic Ulcer Disease and H. pylori Infection". American Family Physician. 91 (4): 236–42. PMID25955624.
↑"Gastritis". The Lecturio Medical Concept Library. Retrieved 22 July 2021.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.