
Varicose veins, also known as varicoses, are a medical condition in which superficial veins become enlarged and twisted. These veins typically develop in the legs, just under the skin. Varicose veins usually cause few symptoms. However, some individuals may experience fatigue or pain in the area. Complications can include bleeding or superficial thrombophlebitis. Varices in the scrotum are known as a varicocele, while those around the anus are known as hemorrhoids. Due to the various physical, social, and psychological effects of varicose veins, they can negatively affect one's quality of life.

The ureters are tubes made of smooth muscle that propel urine from the kidneys to the urinary bladder. In a human adult, the ureters are usually 20–30 cm (8–12 in) long and around 3–4 mm (0.12–0.16 in) in diameter. The ureter is lined by urothelial cells, a type of transitional epithelium, and has an additional smooth muscle layer that assists with peristalsis in its lowest third.

Interventional radiology (IR) is a medical specialty that performs various minimally-invasive procedures using medical imaging guidance, such as x-ray fluoroscopy, computed tomography, magnetic resonance imaging, or ultrasound. IR performs both diagnostic and therapeutic procedures through very small incisions or body orifices. Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct. By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement, and angioplasty of narrowed structures.

Abdominal pain, also known as a stomach ache, Is a symptom associated with both non-serious and serious medical issues. Since the abdomen contains most of the body's vital organs, it can be an indicator of a wide variety of diseases. Given that, approaching the examination of a person and planning of a differential diagnosis is extremely important.
Embolization refers to the passage and lodging of an embolus within the bloodstream. It may be of natural origin (pathological), in which sense it is also called embolism, for example a pulmonary embolism; or it may be artificially induced (therapeutic), as a hemostatic treatment for bleeding or as a treatment for some types of cancer by deliberately blocking blood vessels to starve the tumor cells.

Hydronephrosis describes hydrostatic dilation of the renal pelvis and calyces as a result of obstruction to urine flow downstream. Alternatively, hydroureter describes the dilation of the ureter, and hydronephroureter describes the dilation of the entire upper urinary tract.
Horseshoe kidney, also known as ren arcuatus, renal fusion or super kidney, is a congenital disorder affecting about 1 in 500 people that is more common in men, often asymptomatic, and usually diagnosed incidentally. In this disorder, the patient's kidneys fuse to form a horseshoe-shape during development in the womb. The fused part is the isthmus of the horseshoe kidney. The abnormal anatomy can affect kidney drainage resulting in increased frequency of kidney stones and urinary tract infections as well as increase risk of certain renal cancers.
Renal colic, also known as ureteric colic, is a type of abdominal pain commonly caused by obstruction of ureter from dislodged kidney stones. The most frequent site of obstruction is the vesico-ureteric junction (VUJ), the narrowest point of the upper urinary tract. Acute obstruction and the resultant urinary stasis can distend the ureter (hydroureter) and cause a reflexive peristaltic smooth muscle spasm, which leads to a very intense visceral pain transmitted via the ureteric plexus.

Inferior vena cava syndrome (IVCS) is a very rare constellation of symptoms resulting from either an obstruction, or stenosis of the inferior vena cava. It can be caused by physical invasion or compression by a pathological process or by thrombosis within the vein itself. It can also occur during pregnancy. Pregnancy leads to high venous pressure in the lower limbs, decreased blood return to the heart, decreased cardiac output due to obstruction of the inferior vena cava, sudden rise in venous pressure which can lead to placental separation, and a decrease in kidney function. All of these issues can arise from lying in the supine position during late pregnancy which can cause compression of the inferior vena cava by the uterus. Symptoms of late pregnancy inferior vena cava syndrome consist of intense pain in the right hand side, muscle twitching, hypotension, and fluid retention.

Vesicoureteral reflux (VUR), also known as vesicoureteric reflux, is a condition in which urine flows retrograde, or backward, from the bladder into one or both ureters and then to the renal calyx or kidneys. Urine normally travels in one direction from the kidneys to the bladder via the ureters, with a one-way valve at the vesicoureteral (ureteral-bladder) junction preventing backflow. The valve is formed by oblique tunneling of the distal ureter through the wall of the bladder, creating a short length of ureter (1–2 cm) that can be compressed as the bladder fills. Reflux occurs if the ureter enters the bladder without sufficient tunneling, i.e., too "end-on".
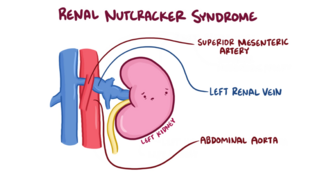
The nutcracker syndrome (NCS) results most commonly from the compression of the left renal vein (LRV) between the abdominal aorta (AA) and superior mesenteric artery (SMA), although other variants exist. The name derives from the fact that, in the sagittal plane and/or transverse plane, the SMA and AA appear to be a nutcracker crushing a nut.

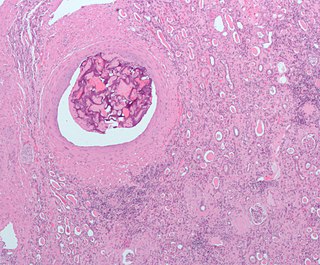
Angiomyolipomas are the most common benign tumour of the kidney. Although regarded as benign, angiomyolipomas may grow such that kidney function is impaired or the blood vessels may dilate and burst, leading to bleeding.

Posterior urethral valve (PUV) disorder is an obstructive developmental anomaly in the urethra and genitourinary system of male newborns. A posterior urethral valve is an obstructing membrane in the posterior male urethra as a result of abnormal in utero development. It is the most common cause of bladder outlet obstruction in male newborns. The disorder varies in degree, with mild cases presenting late due to milder symptoms. More severe cases can have renal and respiratory failure from lung underdevelopment as result of low amniotic fluid volumes, requiring intensive care and close monitoring. It occurs in about one in 8,000 babies.
Pyelogram is a form of imaging of the renal pelvis and ureter.

The pampiniform plexus is a venous plexus – a network of many small veins found in the human male spermatic cord, and the suspensory ligament of the ovary. In the male, it is formed by the union of multiple testicular veins from the back of the testis and tributaries from the epididymis.

Loin pain hematuria syndrome (LPHS) is the combination of debilitating unilateral or bilateral flank pain and microscopic or macroscopic amounts of blood in the urine that is otherwise unexplained.
Bladder outlet obstruction occurs when urine is unable to flow from the kidneys through the ureters and out of the bladder through the urethra. Decreased flow of urine leads to swelling of the urinary tract, called hydronephrosis. This process of decreased flow of urine through the urinary tract can begin as early as during intrauterine life and it prevents normal development of fetal kidneys and fetal urine. Low levels of fetal urine leads to low amniotic fluid levels and incomplete lung maturation. Older children and adults can also experience bladder outlet obstruction; however, this process is usually reversible and isn't associated with as many poor outcomes as in infants with congenital bladder outlet obstruction.

Fraley syndrome is a condition where the superior infundibulum of the upper calyx of the kidney is obstructed by the crossing renal artery branch, causing distension and dilatation of the calyx and presenting clinically as haematuria and nephralgia. Furthermore, when the renal artery obstructs the proximal collecting system, filling defects can occur anywhere in the calyces, pelvis, or ureter.

Pelvic congestion syndrome, also known as pelvic vein incompetence, is a long-term condition believed to be due to enlarged veins in the lower abdomen. The condition may cause chronic pain, such as a constant dull ache, which can be worsened by standing or sex. Pain in the legs or lower back may also occur.
Pelvic compression syndrome is characterized by intermittent or persisting pain in the abdomen, which is exacerbated by abdominal pressure. A swelling of the veins in the valveless pampiniform plexus causes it.
