
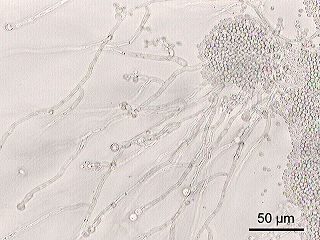
Cryptococcus neoformans is an encapsulated yeast belonging to the class Tremellomycetes and an obligate aerobe that can live in both plants and animals. Its teleomorph is a filamentous fungus, formerly referred to Filobasidiella neoformans. In its yeast state, it is often found in bird excrement. Cryptococcus neoformans can cause disease in apparently immunocompetent, as well as immunocompromised, hosts.

Cryptococcosis is a potentially fatal fungal infection of mainly the lungs, presenting as a pneumonia, and brain, where it appears as a meningitis. Cough, difficulty breathing, chest pain and fever are seen when the lungs are infected. When the brain is infected, symptoms include headache, fever, neck pain, nausea and vomiting, light sensitivity and confusion or changes in behavior. It can also affect other parts of the body including skin, where it may appear as several fluid-filled nodules with dead tissue.
Candida is a genus of yeasts. It is the most common cause of fungal infections worldwide and the largest genus of medically important yeast.
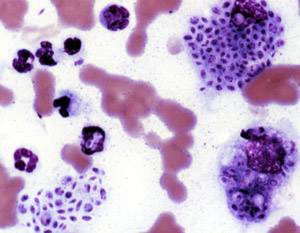
Bartonellosis is an infectious disease produced by bacteria of the genus Bartonella. Bartonella species cause diseases such as Carrión's disease, trench fever, cat-scratch disease, bacillary angiomatosis, peliosis hepatis, chronic bacteremia, endocarditis, chronic lymphadenopathy, and neurological disorders.
Sporotrichosis, also known as rose handler's disease, is a fungal infection that may be localised to skin, lungs, bone and joint, or become systemic. It presents with firm painless nodules that later ulcerate. Following initial exposure to Sporothrix schenckii, the disease typically progresses over a period of a week to several months. Serious complications may develop in people who have a weakened immune system.

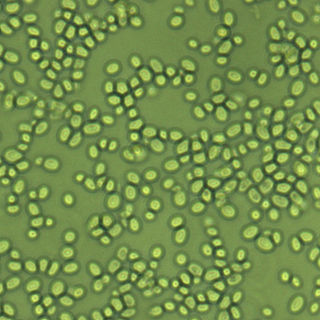
Protothecosis, otherwise known as Algaemia, is a disease found in dogs, cats, cattle, and humans caused by a type of green alga known as Prototheca that lacks chlorophyll and enters the human or animal bloodstream. It and its close relative Helicosporidium are unusual in that they are actually green algae that have become parasites. The two most common species are Prototheca wickerhamii and Prototheca zopfii. Both are known to cause disease in dogs, while most human cases are caused by P. wickerhami. Prototheca is found worldwide in sewage and soil. Infection is rare despite high exposure, and can be related to a defective immune system. In dogs, females and Collies are most commonly affected.
Pichia kudriavzevii is a budding yeast involved in chocolate production. P. kudriavzevii is an emerging fungal nosocomial pathogen primarily found in the immunocompromised and those with hematological malignancies. It has natural resistance to fluconazole, a standard antifungal agent. It is most often found in patients who have had prior fluconazole exposure, sparking debate and conflicting evidence as to whether fluconazole should be used prophylactically. Mortality due to P. kudriavzevii fungemia is much higher than the more common C. albicans. Other Candida species that also fit this profile are C. parapsilosis, C. glabrata, C. tropicalis, C. guillermondii and C. rugosa.
Nakaseomyces glabratus is a species of haploid yeast of the genus Nakaseomyces, previously known as Candida glabrata. Despite the fact that no sexual life cycle has been documented for this species, N. glabratus strains of both mating types are commonly found. N. glabrata is generally a commensal of human mucosal tissues, but in today's era of wider human immunodeficiency from various causes, N. glabratus is often the second or third most common cause of candidiasis as an opportunistic pathogen. Infections caused by N. glabratus can affect the urogenital tract or even cause systemic infections by entrance of the fungal cells in the bloodstream (Candidemia), especially prevalent in immunocompromised patients.

Geotrichum is a genus of fungi found worldwide in soil, water, air, and sewage, as well as in plants, cereals, and dairy products; it is also commonly found in normal human flora and is isolated from sputum and feces. It was first described in 1809 by Johann Heinrich Friedrich Link.

Setosphaeria rostrata is a heat tolerant fungus with an asexual reproductive form (anamorph) known as Exserohilum rostratum. This fungus is a common plant pathogen, causing leaf spots as well as crown rot and root rot in grasses. It is also found in soils and on textiles in subtropical and tropical regions. Exserohilum rostratum is one of the 35 Exserohilum species implicated uncommonly as opportunistic pathogens of humans where it is an etiologic agent of sinusitis, keratitis, skin lesions and an often fatal meningoencephalitis. Infections caused by this species are most often seen in regions with hot climates like Israel, India and the southern USA.

Paracoccidioides brasiliensis is a dimorphic fungus and one of the two species that cause paracoccidioidomycosis. The fungus has been affiliated with the family Ajellomycetaceae although a sexual state or teleomorph has not yet been found.
Lacazia is a genus of fungi containing the single species Lacazia loboi, which is responsible for Lobo's disease. It is a member of the order Onygenales.

Dimorphic fungi are fungi that can exist in the form of both mold and yeast. This is usually brought about by change in temperature and the fungi are also described as thermally dimorphic fungi. An example is Talaromyces marneffei, a human pathogen that grows as a mold at room temperature, and as a yeast at human body temperature.

Blastocystosis refers to a medical condition caused by infection with Blastocystis. Blastocystis is a protozoal, single-celled parasite that inhabits the gastrointestinal tracts of humans and other animals. Many different types of Blastocystis exist, and they can infect humans, farm animals, birds, rodents, amphibians, reptiles, fish, and even cockroaches. Blastocystosis has been found to be a possible risk factor for development of irritable bowel syndrome.

Fonsecaea pedrosoi is a fungal species in the family Herpotrichiellaceae, and the major causative agent of chromoblastomycosis. This species is commonly found in tropical and sub-tropical regions, especially in South America, where it grows as a soil saprotroph. Farming activities in the endemic zone are a risk factor for the development of chromoblastomycosis.

Lichtheimia corymbifera is a thermophilic fungus in the phylum Zygomycota. It normally lives as a saprotrophic mold, but can also be an opportunistic pathogen known to cause pulmonary, CNS, rhinocerebral, or cutaneous infections in animals and humans with impaired immunity.

Rhinocladiella mackenziei is a deeply pigmented mold that is a common cause of human cerebral phaeohyphomycosis. Rhinocladiella mackenziei was believed to be endemic solely to the Middle East, due to the first cases of infection being limited to the region. However, cases of R. mackenziei infection are increasingly reported from regions outside the Middle East. This pathogen is unique in that the majority of cases have been reported from immunologically normal people.

Trichosporon asteroides is an asexual basidiomycetous fungus first described from human skin but now mainly isolated from blood and urine. T. asteroides is a hyphal fungus with a characteristically yeast-like appearance due to the presence of slimy arthroconidia. Infections by this species usually respond to treatment with azoles and amphotericin B.
Arthrographis kalrae is an ascomycetous fungus responsible for human nail infections described in 1938 by Cochet as A. langeronii. A. kalrae is considered a weak pathogen of animals including human restricted to the outermost keratinized layers of tissue. Infections caused by this species are normally responsive to commonly used antifungal drugs with only very rare exceptions.
Sporothrix brasiliensis is a fungus that is commonly found in soil. It is an emerging fungal pathogen that is causing disease in humans and cats mainly in Brazil and other countries in South America.





