Diagnosis is by biopsy and culture, with medical imaging to help determine the extent of disease.[5] It may appear similar to aspergillosis.[17] Treatment is generally with amphotericin B and surgical debridement.[8] Preventive measures include wearing a face mask in dusty areas, avoiding contact with water-damaged buildings, and protecting the skin from exposure to soil such as when gardening or certain outdoor work.[10] It tends to progress rapidly and is fatal in about half of sinus cases and almost all cases of the widespread type.[2][18]
Mucormycosis is usually rare, [8] but is now ~80 times more common in India.[19] People of any age may be affected, including premature infants.[8] The first known case of mucormycosis was possibly the one described by Friedrich Küchenmeister in 1855.[1] The disease has been reported in natural disasters; 2004 Indian Ocean tsunami and the 2011 Joplin tornado.[20] During the COVID-19 pandemic, an association between mucormycosis and COVID-19 has been reported. This association is thought to relate to reduced immune function during the course of the illness and may also be related to glucocorticoid therapy for COVID-19.[4][21] A rise in cases was particularly noted in India.[22]
Classification
Generally, mucormycosis is classified into five main types according to the part of the body affected.[14][23] A sixth type has been described as mucormycosis of the kidney,[1] or miscellaneous, i.e., mucormycosis at other sites, although less commonly affected.[23]
Stomach and intestine (gastrointestinal); more common among young, premature, and low birth weight infants, who have had antibiotics, surgery, or medications that lower the body's ability to fight infection.[14]
Widespread (disseminated); when the infection spreads to other organs via the blood.[14]
Signs and symptoms
Early stages of periorbital mucormycosis
Signs and symptoms of mucormycosis depend on the location in the body of the infection.[6] Infection usually begins in the mouth or nose and enters the central nervous system via the eyes.[5]
If the fungal infection begins in the nose or sinus and extends to brain, symptoms and signs may include one-sided eye pain or headache, and may be accompanied by pain in the face, numbness, fever, loss of smell, a blocked nose or runny nose. The person may appear to have sinusitis.[24] The face may look swollen on one side, with rapidly progressing "black lesions" across the nose or upper inside of mouth. One eye may look swollen and bulging, and vision may be blurred.[6][24][25]
Invasion of the blood vessels can result in thrombosis and subsequent death of surrounding tissue due to a loss of blood supply.[7] Widespread (disseminated) mucormycosis typically occurs in people who are already sick from other medical conditions, so it can be difficult to know which symptoms are related to mucormycosis. People with disseminated infection in the brain can develop changes in mental status or lapse into a coma.[27][28]
The fungal spores are present in the environment, can be found on items such as moldy bread and fruit, and are breathed in frequently, but cause disease only in some people.[5] In addition to being breathed in and deposited in the nose, sinuses, and lungs, the spores can also enter the skin via blood or directly through a cut or open wound, and can also grow in the intestine if eaten.[14][31] Once deposited, the fungus grows branch-like filaments which invade blood vessels, causing clots to form and surrounding tissues to die.[5] Other reported causes include contaminated wound dressings.[5] Mucormycosis has been reported following the use of elastoplast and the use of tongue depressors for holding in place intravenous catheters.[5] Outbreaks have also been linked to hospital bed sheets, negative-pressure rooms, water leaks, poor ventilation, contaminated medical equipment, and building works.[32] One hypothesis suggests that the spread of fungal spores in India could be due to fumes generated from the burning of Mucorales-rich biomass, like cow dung and crop stubble.[33]
Corticosteroids are commonly used in the treatment of COVID-19 and reduce damage caused by the body's own immune response to the virus. They are immunosuppressant and increase blood sugar levels in both diabetic and non-diabetic patients. It is thought that both these effects may contribute to cases of mucormycosis.[34][35][21]
Mechanism
Most people are frequently exposed to Mucorales without developing the disease.[31] Mucormycosis is generally spread by breathing in, eating food contaminated by, or getting spores of molds of the Mucorales type in an open wound.[15] It is not transmitted between people.[14]
The precise mechanism by which diabetics become susceptible is unclear. In vivo, a high sugar level alone does not permit the growth of the fungus, but acidosis alone does.[1][7] People with high sugar levels frequently have high iron levels, also known to be a risk factor for developing mucormycosis.[7] In people taking deferoxamine, the iron removed is captured by siderophores on Rhizopus species, which then use the iron to grow.[36]
Diagnosis
There is no blood test that can confirm the diagnosis.[37] Diagnosis requires identifying the mold in the affected tissue by biopsy and confirming it with a fungal culture.[8] Because the causative fungi occur all around and may therefore contaminate cultures underway, a culture alone is not decisive.[5] Tests may also include culture and direct detection of the fungus in lung fluid, blood, serum, plasma and urine.[20] Blood tests include a complete blood count to look specifically for neutropenia.[37] Other blood tests include iron levels, blood glucose, bicarbonate, and electrolytes.[37] Endoscopic examination of the nasal passages may be needed.[37]
Imaging
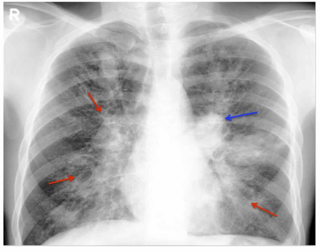
Imaging is often performed, such as CT scan of lungs and sinuses.[38] Signs on chest CT scans, such as nodules, cavities, halo signs, pleural effusion and wedge-shaped shadows, showing invasion of blood vessels, may suggest a fungal infection, but do not confirm mucormycosis.[17] A reverse halo sign in a person with a blood cancer and low neutrophil count is highly suggestive of mucormycosis.[17] CT scan images of mucormycosis can be useful to distinguish mucormycosis of the orbit and cellulitis of the orbit, but images may appear identical to those of aspergillosis.[17]MRI may also be useful.[39] Currently,[when?] MRI with gadolinium contrast is the investigation of choice in rhinoorbito-cerebral mucormycosis.[citation needed]
Culture and biopsy
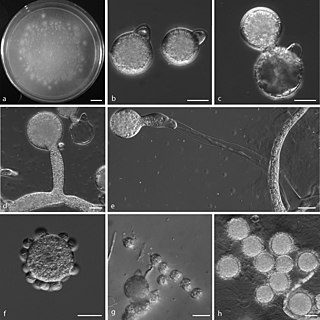
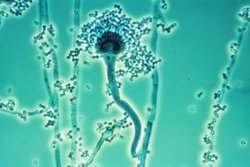
To confirm the diagnosis, biopsy samples can be cultured.[13][37] Culture from biopsy samples does not always give a result as the organism is very fragile.[17] Microscopy can usually determine the genus and sometimes the species, but may require an expert mycologist.[17] The appearance of the fungus under the microscope can vary but generally shows wide (10–20 micron), ribbon-like filaments that generally do not have septa and that—unlike in aspergillosis—branch at right angles, resembling antlers of a moose, which may be seen to be invading blood vessels.[12][37]
Preventive measures include wearing a face mask in dusty areas, washing hands, avoiding direct contact with water-damaged buildings, and protecting skin, feet, and hands where there is exposure to soil or manure, such as gardening or certain outdoor work.[10] In high risk groups, such as organ transplant patients, antifungal drugs may be given as a preventative.[10]
Once mucormycosis is suspected, amphotericin B at an initial dose of 1mg is initially given slowly over 10–15 minutes into a vein, then given as a once daily dose according to body weight for the next 14 days.[43] It may need to be continued for longer.[41]Isavuconazole and Posaconazole are alternatives.[20][44]
Surgery
Surgery can be very drastic, and, in some cases of disease involving the nasal cavity and the brain, removal of infected brain tissue may be required. Removal of the palate, nasal cavity, or eye structures can be very disfiguring.[26] Sometimes more than one operation is required.[31]
Other considerations
The disease must be monitored carefully for any signs of reemergence.[31][45] Treatment also requires correcting sugar levels and improving neutrophil counts.[1][7]Hyperbaric oxygen may be considered as an adjunctive therapy, because higher oxygen pressure increases the ability of neutrophils to kill the fungus.[7] The efficacy of this therapy is uncertain.[32]
Prognosis
It tends to progress rapidly and is fatal in about half of sinus cases, two thirds of lung cases, and almost all cases of the widespread type.[18] Skin involvement carries the lowest mortality rate of around 15%.[31] Possible complications of mucormycosis include the partial loss of neurological function, blindness, and clotting of blood vessels in the brain or lung.[26]
As treatment usually requires extensive and often disfiguring facial surgery, the effect on life after surviving, particularly sinus and brain involvement, is significant.[31]
Epidemiology
The true incidence and prevalence of mucormycosis may be higher than appears.[36] Mucormycosis is rare, affecting fewer than 1.7 people per million population each year in San Francisco.[8][46] It is around 80 times more prevalent in India, where it is estimated that there are around 0.14 cases per 1000 population,[19] and where its incidence has been rising.[47] Causative fungi are highly dependent on location. Apophysomyces variabilis has its highest prevalence in Asia and Lichtheimia spp. in Europe.[20] It is the third most common serious fungal infection to infect people, after aspergillosis and candidiasis.[48]
Diabetes is the main underlying disease in low and middle-income countries, whereas, blood cancers and organ transplantation are the more common underlying problems in developed countries.[19] As new immunomodulating drugs and diagnostic tests are developed, the statistics for mucormycosis have been changing.[19] In addition, the figures change as new genera and species are identified, and new risk factors reported such as tuberculosis and kidney problems.[19]
COVID-19–associated mucormycosis
India
Countries where COVID-associated mucormycosis has been detected as of June 2021
During the COVID-19 pandemic in India, the Indian government reported that more than 11,700 people were receiving care for mucormycosis as of 25 May 2021. Many Indian media outlets called it "black fungus" because of the black discoloration of dead and dying tissue the fungus causes. Even before the COVID-19 pandemic, rates of mucormycosis in India were estimated to be about 70 times higher than in the rest of the world.[3][49] Due to its rapidly growing number of cases some Indian state governments have declared it an epidemic.[50] One treatment was a daily injection for eight weeks of anti-fungal intravenous injection of amphotericin B which was in short supply. The injection could be standard amphotericin B deoxycholate or the liposomal form. The liposomal form cost more but it was considered "safer, more effective and [with] lesser side effects".§[51] The major obstacle of using antifungal drugs in black fungus is the lack of clinical trials.[28]
Recurrence of mucormycosis during COVID-19 second wave in India
Pre-COVID mucormycosis was a very rare infection, even in India. It is so rare that an ENT (ear, nose, throat) doctor would not witness often a case during their university time. So, the documentation available on the treatment of mucormycosis is limited. In fact, there used to be a couple of mucormycosis expert ENT surgeons for millions of people pre-pandemic. The sudden rise in mucormycosis cases has left a majority of the ENT doctors with no option but to accept mucormycosis cases, as the expert doctors were very much occupied and the patient would die if left untreated. The majority of the ENT doctors had to manage with minimal or no experience on mucormycosis, this has led to the recurrence of mucormycosis in the patients they treated. When a highly experienced doctor in mucormycosis treats a patient even he cannot guarantee that the individual is completely cured and will not have a relapse of mucormycosis; an inexperienced ENT surgeon will definitely have a high number of patients with recurrence due to which there were many recurrent cases of mucormycosis although it did not get the limelight of media or the Indian Government.
In 1953, Saksenaea vasiformis, found to cause several cases, was isolated from Indian forest soil, and in 1979, P. C. Misra examined soil from an Indian mango orchard, from where they isolated Apophysomyces, later found to be a major cause of mucormycosis.[1] Several species of mucorales have since been described.[1] When cases were reported in the United States in the mid-1950s, the author thought it to be a new disease resulting from the use of antibiotics, ACTH and steroids.[52][53] Until the latter half of the 20th century, the only available treatment was potassium iodide. In a review of cases involving the lungs diagnosed following flexible bronchoscopy between 1970 and 2000, survival was found to be better in those who received combined surgery and medical treatment, mostly with amphotericin B.[52]
Naming
Arnold Paltauf coined the term "Mycosis Mucorina" in 1885, after describing a case with systemic symptoms involving the sinus, brain and gastrointestinal tract, following which the term "mucormycosis" became popular.[1] "Mucormycosis" is often used interchangeably with "zygomycosis", a term made obsolete following changes in classification of the kingdomFungi. The former phylumZygomycota included Mucorales, Entomophthorales, and others. Mucormycosis describes infections caused by fungi of the order Mucorales.[41]
COVID-19–associated mucormycosis
COVID-19 associated mucormycosis cases were reported during first and second(delta) wave, with maximum number of cases in delta wave.[11] There were no cases reported during the Omicron wave.[11] A number of cases of mucormycosis, aspergillosis, and candidiasis, linked to immunosuppressive treatment for COVID-19 were reported during the COVID-19 pandemic in India in 2020 and 2021.[4][39] One review in early 2021 relating to the association of mucormycosis and COVID-19 reported eight cases of mucormycosis; three from the U.S., two from India, and one case each from Brazil, Italy, and the UK.[21] The most common underlying medical condition was diabetes.[21] Most had been in hospital with severe breathing problems due to COVID-19, had recovered, and developed mucormycosis 10–14 days following treatment for COVID-19. Five had abnormal kidney function tests, three involved the sinus, eye and brain, three the lungs, one the gastrointestinal tract, and in one the disease was widespread.[21] In two of the seven deaths, the diagnosis of mucormycosis was made at postmortem.[21] That three had no traditional risk factors led the authors to question the use of steroids and immunosuppressive drugs.[21] Although, there were cases without diabetes or use of immunosuppressive drugs. There were cases reported even in children.[11] In May 2021, the BBC reported increased cases in India.[34] In a review of COVID-19-related eye problems, mucormycosis affecting the eyes was reported to occur up to several weeks following recovery from COVID-19.[39] It was observed that people with COVID-19 were recovering from mucormycosis a bit easily when compared to non-COVID-19 patients. This is because unlike non-COVID-19 patients with severe diabetes, cancer or HIV, the recovery time required for the main cause of immune suppression is temporary.[11]
Other countries affected included Pakistan,[54] Nepal,[55] Bangladesh,[56] Russia,[57] Uruguay,[58] Paraguay,[59] Chile,[60] Egypt,[61] Iran,[62] Brazil,[63] Iraq,[64] Mexico,[65] Honduras,[66] Argentina[67] Oman,[68] and Afghanistan.[69] One explanation for why the association has surfaced remarkably in India is high rates of COVID-19 infection and high rates of diabetes.[70] In May 2021, the Indian Council of Medical Research issued guidelines for recognising and treating COVID-19–associated mucormycosis.[71] In India, as of 28 June 2021, over 40,845 people have been confirmed to have mucormycosis, and 3,129 have died. From these cases, 85.5% (34,940) had a history of being infected with SARS-CoV-2 and 52.69% (21,523) were on steroids, also 64.11% (26,187) had diabetes.[72][73]
Society and culture
The disease has been reported in natural disasters and catastrophes; 2004 Indian Ocean tsunami and the 2011 Missouri tornado.[20][74] The first international congress on mucormycosis was held in Chicago in 2010, set up by the Hank Schueuler 41 & 9 Foundation, which was established in 2008 for the research of children with leukaemia and fungal infections.[1] A cluster of infections occurred in the wake of the 2011 Joplin tornado. By July 19, 2011, a total of 18suspected cases of mucormycosis of the skin had been identified, of which 13 were confirmed. A confirmed case was defined as 1) necrotizing soft-tissue infection requiring antifungal treatment or surgical debridement in a person injured in the tornado, 2) with illness onset on or after May 22 and 3) positive fungal culture or histopathology and genetic sequencing consistent with a mucormycete. No additional cases related to that outbreak were reported after June 17. Ten people required admission to an intensive-care unit, and five died.[75][76]
In 2014, details of a lethal mucormycosis outbreak that occurred in 2008 emerged after television and newspaper reports responded to an article in a pediatric medical journal.[77][78] Contaminated hospital linen was found to be spreading the infection. A 2018 study found many freshly laundered hospital linens delivered to U.S. transplant hospitals were contaminated with Mucorales.[79] Another study attributed an outbreak of hospital-acquired mucormycosis to a laundry facility supplying linens contaminated with Mucorales. The outbreak stopped when major changes were made at the laundry facility. The authors raised concerns on the regulation of healthcare linens.[80]
Other animals
Mucormycosis in other animals is similar, in terms of frequency and types, to that in people.[81] Cases have been described in cats, dogs, cows, horses, dolphins, bison, and seals.[81]
Related Research Articles
Zygomycosis is the broadest term to refer to infections caused by bread mold fungi of the zygomycota phylum. However, because zygomycota has been identified as polyphyletic, and is not included in modern fungal classification systems, the diseases that zygomycosis can refer to are better called by their specific names: mucormycosis, phycomycosis and basidiobolomycosis. These rare yet serious and potentially life-threatening fungal infections usually affect the face or oropharyngeal cavity. Zygomycosis type infections are most often caused by common fungi found in soil and decaying vegetation. While most individuals are exposed to the fungi on a regular basis, those with immune disorders (immunocompromised) are more prone to fungal infection. These types of infections are also common after natural disasters, such as tornadoes or earthquakes, where people have open wounds that have become filled with soil or vegetative matter.
Aspergillus is a genus consisting of several hundred mold species found in various climates worldwide.
Fungal infection, also known as mycosis, is a disease caused by fungi. Different types are traditionally divided according to the part of the body affected; superficial, subcutaneous, and systemic. Superficial fungal infections include common tinea of the skin, such as tinea of the body, groin, hands, feet and beard, and yeast infections such as pityriasis versicolor. Subcutaneous types include eumycetoma and chromoblastomycosis, which generally affect tissues in and beneath the skin. Systemic fungal infections are more serious and include cryptococcosis, histoplasmosis, pneumocystis pneumonia, aspergillosis and mucormycosis. Signs and symptoms range widely. There is usually a rash with superficial infection. Fungal infection within the skin or under the skin may present with a lump and skin changes. Pneumonia-like symptoms or meningitis may occur with a deeper or systemic infection.
Fungal pneumonia is an infection of the lungs by fungi. It can be caused by either endemic or opportunistic fungi or a combination of both. Case mortality in fungal pneumonias can be as high as 90% in immunocompromised patients, though immunocompetent patients generally respond well to anti-fungal therapy.
An aspergilloma is a clump of mold which exists in a body cavity such as a paranasal sinus or an organ such as the lung. By definition, it is caused by fungi of the genus Aspergillus.
Phycomycosis is an uncommon condition of the gastrointestinal tract and skin most commonly found in dogs and horses. The condition is caused by a variety of molds and fungi, and individual forms include pythiosis, zygomycosis, and lagenidiosis. Pythiosis is the most common type and is caused by Pythium, a type of water mould. Zygomycosis can also be caused by two types of zygomycetes, Entomophthorales and Mucorales. The latter type of zygomycosis is also referred to as mucormycosis. Lagenidiosis is caused by a Lagenidium species, which like Pythium is a water mould. Since both pythiosis and lagenidiosis are caused by organisms from the Oomycetes and not the kingdom fungi, they are sometimes collectively referred to as oomycosis.
Allergic bronchopulmonary aspergillosis (ABPA) is a condition characterised by an exaggerated response of the immune system to the fungus Aspergillus. It occurs most often in people with asthma or cystic fibrosis. Aspergillus spores are ubiquitous in soil and are commonly found in the sputum of healthy individuals. A. fumigatus is responsible for a spectrum of lung diseases known as aspergilloses.
Aspergillosis is a fungal infection of usually the lungs, caused by the genus Aspergillus, a common mould that is breathed in frequently from the air, but does not usually affect most people. It generally occurs in people with lung diseases such as asthma, cystic fibrosis or tuberculosis, or COVID-19 or those who are immunocompromized such as those who have had a stem cell or organ transplant or those who take medications such as steroids and some cancer treatments which suppress the immune system. Rarely, it can affect skin.
Apophysomyces is a genus of filamentous fungi that are commonly found in soil and decaying vegetation. Species normally grow in tropical to subtropical regions.
Conidiobolomycosis is a rare long-term fungal infection that is typically found just under the skin of the nose, sinuses, cheeks and upper lips. It may present with a nose bleed or a blocked or runny nose. Typically there is a firm painless swelling which can slowly extend to the nasal bridge and eyes, sometimes causing facial disfigurement.
Pathogenic fungi are fungi that cause disease in humans or other organisms. Although fungi are eukaryotic, many pathogenic fungi are microorganisms. Approximately 300 fungi are known to be pathogenic to humans; their study is called "medical mycology". Fungal infections are estimated to kill more people than either tuberculosis or malaria—about two million people per year.
Saksenaea vasiformis is an infectious fungus associated with cutaneous or subcutaneous lesions following trauma. It causes opportunistic infections as the entry of the fungus is through open spaces of cutaneous barrier ranging in severity from mild to severe or fatal. It lives in soils worldwide, but is considered as a rare human pathogen since only 38 cases were reported as of 2012. Saksenaea vasiformis usually fails to sporulate on the routine culture media, creating a challenge for early diagnosis, which is essential for a good prognosis. Infections are usually treated using a combination of amphotericin B and surgery. Saksenaea vasiformis is one of the few fungi known to cause necrotizing fasciitis or "flesh-eating disease".
Rhizomucor pusillus is a species of Rhizomucor. It can cause disease in humans. R. pusillus is a grey mycelium fungi most commonly found in compost piles. Yellow-brown spores grow on a stalk to reproduce more fungal cells.
Chronic pulmonary aspergillosis is a long-term fungal infection caused by members of the genus Aspergillus—most commonly Aspergillusfumigatus. The term describes several disease presentations with considerable overlap, ranging from an aspergilloma—a clump of Aspergillus mold in the lungs—through to a subacute, invasive form known as chronic necrotizing pulmonary aspergillosis which affects people whose immune system is weakened. Many people affected by chronic pulmonary aspergillosis have an underlying lung disease, most commonly tuberculosis, allergic bronchopulmonary aspergillosis, asthma, or lung cancer.
Apophysomyces variabilis is an emerging fungal pathogen that can cause serious and sometimes fatal infection in humans. This fungus is a soil-dwelling saprobe with tropical to subtropical distribution. It is a zygomycete that causes mucormycosis, an infection in humans brought about by fungi in the order Mucorales. Infectious cases have been reported globally in locations including the Americas, Southeast Asia, India, and Australia. Apophysomyces variabilis infections are not transmissible from person to person.
Lichtheimia corymbifera is a thermophilic fungus in the phylum Zygomycota. It normally lives as a saprotrophic mold, but can also be an opportunistic pathogen known to cause pulmonary, CNS, rhinocerebral, or cutaneous infections in animals and humans with impaired immunity.
Cunninghamella bertholletiae is a species of zygomycetous fungi in the order Mucorales. It is found globally, with increased prevalence in Mediterranean and subtropical climates. It typically grows as a saprotroph and is found in a wide variety of substrates, including soil, fruits, vegetables, nuts, crops, and human and animal waste. Although infections are still rare, C. betholletiae is emerging as an opportunistic human pathogen, predominantly in immunocompromised people, leukemia patients, and people with uncontrolled diabetes. Cunninghamella bertholletiae infections are often highly invasive, and can be more difficult to treat with antifungal drugs than infections with other species of the Mucorales, making prompt and accurate recognition and diagnosis of mycoses caused by this fungus an important medical concern.
Fungal sinusitis or fungal rhinosinusitis is the inflammation of the lining mucosa of the paranasal sinuses due to a fungal infection. It occurs in people with reduced immunity. The maxillary sinus is the most commonly involved. Fungi responsible for fungal sinusitis are Aspergillus fumigatus (90%), Aspergillus flavus, and Aspergillus niger. Fungal sinusitis occurs most commonly in middle-aged populations. Diabetes mellitus is the most common risk factor involved.
Mycotypha microspora, also known as Microtypha microspora, is a filamentous fungus in the division Zygomycota. It was discovered in a Citrus aurantium peel in 1932 by E. Aline Fenner, who proposed a new genus Mycotypha to accommodate it. Mycotypha africana, which is another species in the genus Mycotypha, is closely related to M. microspora. The fungus has subsequently been isolated from both outdoor and indoor settings around the world, and is typically found in soil and dung. The species rarely causes infections in humans, but has recently been involved in the clinical manifestation of the life-threatening disease mucormycosis.
Akshay Nair is an Indian ophthalmologist based in Mumbai, India. He specializes in oculoplastics, orbital surgery and ocular oncology. Currently, Dr. Nair is the Director of Ophthalmic plastic surgery and ocular oncology services at the Mumbai units of Dr. Agarwal's Eye Hospital: Advanced Eye Hospital and Institute and Aditya Jyot Eye Hospital.
1 2 Riley TT, Muzny CA, Swiatlo E, Legendre DP (September 2016). "Breaking the Mold: A Review of Mucormycosis and Current Pharmacological Treatment Options". The Annals of Pharmacotherapy. 50 (9): 747–57. doi:10.1177/1060028016655425. PMID27307416. S2CID22454217.
↑ Lewis RE, Kontoyiannis DP (September 2013). "Epidemiology and treatment of mucormycosis". Future Microbiology. 8 (9): 1163–75. doi:10.2217/fmb.13.78. PMID24020743.
↑ Vallabhaneni S, Mody RK, Walker T, Chiller T (2016). "1. The global burden of fungal disease". In Sobel J, Ostrosky-Zeichner L (eds.). Fungal Infections, An Issue of Infectious Disease Clinics of North America. Philadelphia: Elsevier. pp.5–12. ISBN978-0-323-41649-8.
↑ "5 Children's Hospital patients died in 2008, 2009 after contact with deadly fungus". We acknowledge that Children's Hospital is Hospital A in an upcoming article in The Pediatric Infectious Disease Journal. The safety and well-being of our patients are our top priorities, so as soon as a problem was suspected, the State Health Department and CDC were notified and invited to assist in the investigation. The hospital was extremely aggressive in trying to isolate and then eliminate the source of the fungus.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.