Nankali’s masticatory force systematization categorizes the locations of the forces on different part of mandible/maxilla, which are important in designing a prosthetic and implant treatment in dentistry.
Contents

Nankali’s masticatory force systematization categorizes the locations of the forces on different part of mandible/maxilla, which are important in designing a prosthetic and implant treatment in dentistry.
The muscles of mastication or masticatory muscles are: [1]
Masticatory force or force of mastication is defined as the force that is created by the dynamic action of the masticatory muscles during the act of chewing.
The masticatory force initially was measured by Dr. Bleck. Bleck used a gnathodynamometer and also found out the close relation between periodontal tissue and masticatory force.
A gnathodynamometer is an instrument for measuring the force exerted in closing the mouth. A bimeter gnathodynamometer is one with an adjustable central-bearing point.

Dr. Morill worked more deeply on the relationship between masticatory muscles and pain signals from the periodontal tissue in different ways. [2]
Dr. Shreder, using local anaesthesia (to ignore the periodontal response) measured the maximum possible force of the masticatory system and discovered the differences in the produced force, which was approximately doubled. [3]
The periodontal system controls automatically the measure of mastication force in this process and the jaw elevator muscles develop the main forces used in mastication.
Dr. Weber worked out that 1 cm2 cross section surface area of any masticatory muscle can produce approximately 10 kg force. The following average surfaces were found: [4] temporalis - 8 cm2, masseter - 7.5 cm2, and medial pterygoid - 4 cm2 which makes a total of 19.5cm2. However, this force in some people is measured up to 3900N in combination.

In human anatomy, the masseter is one of the muscles of mastication. Found only in mammals, it is particularly powerful in herbivores to facilitate chewing of plant matter. The most obvious muscle of mastication is the masseter muscle, since it is the most superficial and one of the strongest.

The medial pterygoid, is a thick, quadrilateral muscle of mastication.
The force generated during routine mastication like having carrots or meat is about 70-150N although in some people with specific conditions it may reach up to 500-700N.; [5]
Dr. Ali Nankali continued the masticatory force study and observed a number of mastication acts by individuals using computer. The monitored results of this investigation illustrated constant changes in the amount of masticatory force during mastication [6] due to the characteristic and size of the mouthful.
He also studied the relation between mechanical and bio-physiological movements of the masticatory system which shows that creating the masticatory force is directly depended to the surface area and its orientation and therefore he suggested the masticatory force systematization.
According to this systematization, the masticatory force is divided in two main groups, physiological and pathological groups. The physiological masticatory force by itself is divided into three subgroups according to their localizations, anterior, general (covering the entire arch) and posterior section of the arch. The posterior group is also divided into two other groups; unilateral and bilateral. [7]
This systematization proves that the condition of producing a maximum masticatory force by a person is using the general subgroup of this systematization.
The systematization of the masticatory force distribution was designed by Nankali in the National Medical University at the orthopedic and implant stomatology department, which was verified (October 1999) by the Scientific Board of National Medical University (O.O. Bogomolets) and international patent organization (УДК; 616.314-76-77:616.314.11-74:678.029.46:612.311) in Kiev.
This systematization was presented for the first time at the 55th Medical Science Conference of Students & Young Scientists in 2000, organized by the Ukraine Health Ministry and the National Medical University known as O.O. Bogomolets, and Society Science Students known as O.O. Kisilia. The result of presentation in "Young Scientists and Students / Scientific Medical Seminar in 1999" was published.
Temporomandibular joint dysfunction is an umbrella term covering pain and dysfunction of the muscles of mastication and the temporomandibular joints. The most important feature is pain, followed by restricted mandibular movement, and noises from the temporomandibular joints (TMJ) during jaw movement. Although TMD is not life-threatening, it can be detrimental to quality of life, because the symptoms can become chronic and difficult to manage.

The tongue is a muscular organ in the mouth of most vertebrates that manipulates food for mastication, and is used in the act of swallowing. It is of importance in the digestive system and is the primary organ of taste in the gustatory system. The tongue's upper surface (dorsum) is covered by taste buds housed in numerous lingual papillae. It is sensitive and kept moist by saliva, and is richly supplied with nerves and blood vessels. The tongue also serves as a natural means of cleaning the teeth. A major function of the tongue is the enabling of speech in humans and vocalization in other animals.

Inflammation is part of the complex biological response of body tissues to harmful stimuli, such as pathogens, damaged cells, or irritants, and is a protective response involving immune cells, blood vessels, and molecular mediators. The function of inflammation is to eliminate the initial cause of cell injury, clear out necrotic cells and tissues damaged from the original insult and the inflammatory process, and initiate tissue repair.
Periodontal disease, also known as gum disease, is a set of inflammatory conditions affecting the tissues surrounding the teeth. In its early stage, called gingivitis, the gums become swollen, red, and may bleed. In its more serious form, called periodontitis, the gums can pull away from the tooth, bone can be lost, and the teeth may loosen or fall out. Bad breath may also occur.

Bruxism is excessive teeth grinding or jaw clenching. It is an oral parafunctional activity; i.e., it is unrelated to normal function such as eating or talking. Bruxism is a common behavior; reports of prevalence range from 8% to 31% in the general population. Several symptoms are commonly associated with bruxism, including hypersensitive teeth, aching jaw muscles, headaches, tooth wear, and damage to dental restorations to teeth. But symptoms may be minimal, without patient awareness of the condition.
The temporomandibular joints (TMJ) are the two joints connecting the jawbone to the skull. It is a bilateral synovial articulation between the temporal bone of the skull above and the mandible below; it is from these bones that its name is derived. This joint is unique in that it is a bilateral joint that functions as one unit. Since the TMJ is connected to the mandible, the right and left joints must function together and therefore are not independent of each other.
Trismus, also called lockjaw, is reduced opening of the jaws. It may be caused by spasm of the muscles of mastication or a variety of other causes. Temporary trismus occurs much more frequently than permanent trismus. It is known to interfere with eating, speaking, and maintaining proper oral hygiene. This interference, specifically with the patient's ability to swallow properly, results in an increased risk of aspiration. In some instances, trismus presents with altered facial appearance. The condition may be distressing and painful for the patient. Examination and treatments requiring access to the oral cavity can be limited, or in some cases impossible, due to the nature of the condition itself.

The mandibular nerve (V3) is the largest of the three divisions of the trigeminal nerve, the fifth cranial nerve (CN V).
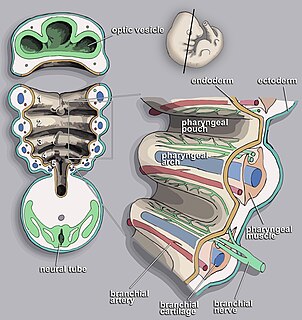
The pharyngeal arches —also known as visceral arches—are structures seen in the embryonic development of vertebrates that are recognisable precursors for many structures. In fish the arches are known as the branchial arches or gill arches.

George Miller Beard was an American neurologist who popularized the term neurasthenia, starting around 1869.
Oropharyngeal dysphagia arises from abnormalities of muscles, nerves or structures of the oral cavity, pharynx, and upper esophageal sphincter.

The deep cervical fascia lies under cover of the platysma, and invests the muscles of the neck; it also forms sheaths for the carotid vessels, and for the structures situated in front of the vertebral column. Its attachment to the hyoid bone prevents the formation of a dewlap.
Occlusion, in a dental context, means simply the contact between teeth. More technically, it is the relationship between the maxillary (upper) and mandibular (lower) teeth when they approach each other, as occurs during chewing or at rest.
Durophagy is the eating behavior of animals that consume hard-shelled or exoskeleton bearing organisms, such as corals, shelled mollusks, or crabs. It is mostly used to describe fish, but is also used when describing reptiles, including fossil turtles, placodonts and invertebrates, as well as "bone-crushing" mammalian carnivores such as hyenas. Durophagy requires special adaptions, such as blunt, strong teeth and a heavy jaw. Bite force is necessary to overcome the physical constraints of consuming more durable prey and gain a competitive advantage over other organisms by gaining access to more diverse or exclusive food resources earlier in life. Those with greater bite forces require less time to consume certain prey items as a greater bite force can increase the net rate of energy intake when foraging and enhance fitness in durophagous species. In the order Carnivora there are two dietary categories of durophagy; bonecrackers and bamboo eaters. Bonecrackers are exemplified by hyenas and saber-toothed cats, while bamboo eaters are primarily the giant panda and the red panda. Both have developed similar cranial morphology. However, the mandible morphology reveals more about their dietary resources. Both have a raised and dome-like anterior cranium, enlarged areas for the attachment of masticatory muscles, enlarged premolars, and reinforced tooth enamel. Bamboo eaters tend to have larger mandibles, while bonecrackers have more sophisticated premolars.

The Nankali post system is a post and cores prosthesis, which is used in prosthodontology and dental restoration. This post and core consists of a single smooth or serrated post and core which has an additional circle ring around it.
The Nankali post and core classification is the most advanced classification that is used in restorative dentistry for grouping different types of post and cores.

Bogomoletz Institute of Physiology of NAS of Ukraine (BIPH) is a scientific institution dedicated to biomedical research in the fields of physiology, biophysics, pathophysiology, neuroscience. It is a leading research center in Ukraine for neuroscience, electrophysiology and cardiovascular diseases.
Vasily Nikolayevich Krylov was a Russian scientist, Doctor of Biological Sciences, Distinguished Professor at the N. I. Lobachevsky State University of Nizhny Novgorod (UNN), Chairman of the Russian Apitherapy Coordinating Council, Honored Scientist of the Russian Federation (2007) and Honorary Worker of Higher Professional Education the Russian Federation. Laureate of the 2016 Nizhny Novgorod Prize. He is known as a bee venom expert.
A complete denture is a removable appliance used when all teeth within a jaw have been lost and need to be prosthetically replaced. In contrast to a partial denture, a complete denture is constructed when there are no more teeth left in an arch, hence it is an exclusively tissue-supported prosthesis. A complete denture can be opposed by natural dentition, a partial or complete denture, fixed appliances or, sometimes, soft tissues.