 Testosterone levels in relation to estradiol levels (and corresponding estradiol dosages) during therapy with oral estradiol alone or in combination with an antiandrogen in transgender women. [92] Dashed purple line is upper limit for female/castrate range (~50 ng/dL) and dashed grey line is testosterone level in a comparison group of post-operative transgender women (21.7 pg/mL). [92]
Testosterone levels in relation to estradiol levels (and corresponding estradiol dosages) during therapy with oral estradiol alone or in combination with an antiandrogen in transgender women. [92] Dashed purple line is upper limit for female/castrate range (~50 ng/dL) and dashed grey line is testosterone level in a comparison group of post-operative transgender women (21.7 pg/mL). [92]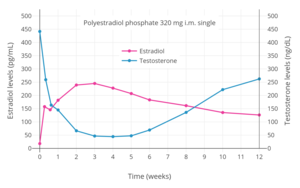 Estradiol and testosterone levels over the course of 12 weeks following a single intramuscular injection of 320 mg polyestradiol phosphate in men with prostate cancer. [81]
Estradiol and testosterone levels over the course of 12 weeks following a single intramuscular injection of 320 mg polyestradiol phosphate in men with prostate cancer. [81] Estradiol and testosterone levels with polyestradiol phosphate 160, 240, or 320 mg once every 4 weeks by intramuscular injection in men with prostate cancer. [105]
Estradiol and testosterone levels with polyestradiol phosphate 160, 240, or 320 mg once every 4 weeks by intramuscular injection in men with prostate cancer. [105]
 Estradiol, testosterone, and prolactin levels with 100 mg/month estradiol undecylate by intramuscular injection in men with prostate cancer. [108]
Estradiol, testosterone, and prolactin levels with 100 mg/month estradiol undecylate by intramuscular injection in men with prostate cancer. [108]






Differences from other estrogens


Estradiol has relatively low oral bioavailability of about 5%. [1] In addition, there is considerable interindividual variability in levels of estradiol achieved with oral estradiol. [1] In contrast to estradiol, the synthetic estrogen ethinylestradiol has about 45% oral bioavailability, around 80- to 200-fold greater systemic oral estrogenic potency, roughly 500- to 1,500-fold greater hepatic oral estrogenic potency, and less interindividual variability in circulating estrogen levels achieved. [68] [1] [147] [148] [149] [150] [151] An oral dose of ethinylestradiol that is approximately 100-fold lower than that of estradiol achieves similar maximal circulating estrogen concentrations (e.g., 50 pg/mL ethinylestradiol with a single 20 μg dose of ethinylestradiol relative to 40 pg/mL estradiol with a single 2 mg dose of micronized estradiol or estradiol valerate). [1] These differences are due to the introduction of an ethynyl group at the C17α position in ethinylestradiol (also known as 17α-ethynylestradiol), which results in steric hindrance and greatly diminishes the first-pass metabolism of ethinylestradiol relative to estradiol with oral administration. [1] Estradiol and ethinylestradiol have similar affinities for and efficacies as agonists of the ERs, [1] [2] and the systemic estrogenic potency of estradiol and ethinylestradiol is similar when they are administered by the intravenous route. [152]
Synthetic estrogens like ethinylestradiol and diethylstilbestrol and the natural but animal-derived conjugated estrogens have disproportionate effects on liver protein synthesis relative to their effects in other tissues when compared to estradiol. [1] At doses via the oral route with comparable systemic estrogenic potency, conjugated estrogens have about 1.3 to 4.5 times the hepatotropic potency (i.e., potency in modulating liver protein synthesis) of estradiol, ethinylestradiol has about 2.9 to 5.0 times the hepatotropic potency of estradiol, and diethylstilbestrol shows about 5.7 to 7.5 times the hepatotropic potency of estradiol (all measured via a small selection of estrogen-modulated hepatic proteins that included HDL cholesterol, SHBG , CBG , and angiotensinogen). [1] The greater hepatotropic potency of these estrogens relative to estradiol is related to susceptibility to hepatic metabolism. [1] Whereas estradiol is metabolized and thereby inactivated rapidly upon entry into the liver, other estrogens like ethinylestradiol and diethylstilbestrol are resistant to hepatic metabolism and persist in the liver for a longer amount of time. [1] This is reflected in the biological half-lives of these estrogens; the blood half-life of estradiol is about 1 to 2 hours, while the half-lives of ethinylestradiol and diethylstilbestrol are approximately 20 hours and 24 hours, respectively. [153] [154] [151] In accordance with its long half-life, ethinylestradiol passes through the liver many times prior to its elimination. [155] Because humans are not adapted to efficiently metabolize conjugated estrogens (which are equine (horse) estrogens) and synthetic estrogens like ethinylestradiol and diethylstilbestrol, these estrogens are not properly inactivated in the liver, with markedly disproportionate hepatic estrogenic effects resulting. [1]
In addition to differences in hepatotropic potency between estradiol and other estrogens, there are differences in hepatotropic potency between different routes of administration of estradiol. [1] Due to the first pass through the liver, oral estradiol results in disproportionate and unphysiological hepatic estradiol levels that are 4- to 5-fold higher than in the circulation. [156] [1] Conversely, parenteral routes of estradiol, such as transdermal, vaginal, and injection, bypass the first pass through the liver and produce levels of estradiol in the circulation and liver that are comparable. [156] [1] As an example of the reduced hepatic impact of parenteral estradiol relative to oral estradiol, a study found that 1 mg/day oral estradiol significantly increased SHBG levels by 45%, while 50 µg/day transdermal estradiol increased SHBG levels non-significantly by only 12% (with these dosages being roughly equivalent in systemic estrogenic potency). [157] [158] [159] As such, not only do oral non-bioidentical estrogens like ethinylestradiol and conjugated estrogens have substantially greater potency in the liver than does oral estradiol, oral estradiol has considerably greater potency in the liver than does parenteral estradiol. [1] Thus, the hepatotropic effects of oral non-bioidentical estrogens like ethinylestradiol are massive in comparison to parenteral estradiol (see the graph above/to the right), which in contrast to these estrogens has very weak or even absent effects on liver protein synthesis at normal therapeutic dosages. [1] [81] [68] [3] Whereas high-dosage 320 mg/month intramuscular polyestradiol phosphate increased SHBG levels to 166% in men with prostate cancer, the combination of 80 mg/month intramuscular polyestradiol phosphate and high-dosage 150 µg/day oral ethinylestradiol increased levels of SHBG to 617%, an almost 8-fold difference in increase and almost 4-fold difference in absolute levels between the two treatment regimens. [4] [81] [160]
The effects of estrogens on liver protein synthesis, such as on the synthesis of coagulation factors, lipoproteins, and triglycerides, can cause an increased risk of thromboembolic and cardiovascular complications, which in turn can result in increased mortality. [68] The risk of thromboembolic and cardiovascular complications is significantly increased in postmenopausal women taking oral conjugated estrogens as a component of menopausal hormone therapy. [1] [161] [162] Both oral estradiol and oral esterified estrogens have been found to have a significantly lower risk of thromboembolic and cardiovascular complications than oral conjugated estrogens, and transdermal estradiol appears to have no such risks at all. [1] [163] [161] [162] Widely employed in the past, oral synthetic estrogens like ethinylestradiol and diethylstilbestrol are no longer used in menopausal hormone therapy due to their high risks of thromboembolic and cardiovascular complications. [164] Studies have found a markedly increased 5-year risk of cardiovascular mortality of 14 to 26% in men treated with high-dosage oral synthetic estrogens like ethinylestradiol and diethylstilbestrol for prostate cancer. [68] With diethylstilbestrol, there is an up to 35% incidence of cardiovascular toxicity and an up to 15% incidence of venous thromboembolism. [165] In a small study comparing high-dosage 320 mg/month intramuscular polyestradiol phosphate versus the combination of 80 mg/month polyestradiol phosphate with high-dosage 150 µg/day oral ethinylestradiol for prostate cancer, there was a 25% incidence of cardiovascular complications over the course of a year in the group that was also treated with ethinylestradiol, whereas there were no cardiovascular complications in the polyestradiol phosphate-only group. [81] In accordance, another study found no change in levels of coagulation factor VII, a protein of particular importance in the cardiovascular side effects of estrogens, with 240 mg/month intramuscular polyestradiol phosphate. [166] In spite of the markedly reduced impact of parenteral estradiol on the liver compared to other estrogens however, high dosages of parenteral estradiol, producing high levels of circulating estradiol, can still result in important and undesirable changes in liver protein synthesis as with other estrogens. [40] A high dosage of 320 mg/month polyestradiol phosphate has been found to result in significantly increased cardiovascular morbidity (due to non-fatal ischemic heart events and heart decompensation) in men with prostate cancer in two large studies, though cardiovascular mortality was notably not increased. [40] [167]
In addition to the liver, ethinylestradiol shows disproportionate estrogenic effects in the uterus. [1] [43] [168] This is due to its inability to be inactivated by uterine 17β-hydroxysteroid dehydrogenase (17β-HSD). [1] [43] [168] Because of its disproportionate effects in the uterus, ethinylestradiol is associated with a significantly lower incidence of vaginal bleeding and spotting than is estradiol, particularly in combination with progestogens (which induce 17β-HSD expression and hence estradiol metabolism in the uterus), [1] and is an important contributing factor in why ethinylestradiol, among other reasons and in spite of its inferior safety profile, has been widely used in oral contraceptives instead of estradiol. [132] [131] Although ethinylestradiol has increased effects in the uterus relative to estradiol, it is similarly not associated with an increase in the risk of endometrial hyperplasia and endometrial cancer when used in combination with a progestogen, but instead with a significant decrease. [1] [169]