Endoscopic thoracic sympathectomy (ETS) is a surgical procedure in which a portion of the sympathetic nerve trunk in the thoracic region is destroyed.[1][2] ETS is used to treat excessive sweating in certain parts of the body (focal hyperhidrosis), facial flushing, Raynaud's disease and reflex sympathetic dystrophy. By far the most common complaint treated with ETS is sweaty palms (palmar hyperhidrosis). The intervention is controversial and illegal in some jurisdictions. Like any surgical procedure, it has risks; the endoscopic sympathetic block (ESB) procedure and those procedures that affect fewer nerves have lower risks.
Sympathectomy physically destroys relevant nerves anywhere in either of the two sympathetic trunks, which are long chains of nerve ganglia located bilaterally along the vertebral column (a localisation which entails a low risk of injury) responsible for various important aspects of the peripheral nervous system (PNS). Each nerve trunk is broadly divided into three regions: cervical (neck), thoracic (chest), and lumbar (lower back). The most common area targeted in sympathectomy is the upper thoracic region, that part of the sympathetic chain lying between the first and fifth thoracic vertebrae.
Indications
The most common indications for thoracic sympathectomy are focal hyperhidrosis (that specifically affects the hands and underarms), Raynaud syndrome, and facial blushing when accompanied by focal hyperhidrosis. It may also be used to treat bromhidrosis,[3] although this usually responds to non-surgical treatments,[4] and sometimes people with olfactory reference syndrome present to surgeons requesting sympathectomy.[5]
There are reports of ETS being used to achieve cerebral revascularization for people with moyamoya disease,[6] and to treat headaches, hyperactive bronchial tubes,[7]long QT syndrome,[8][9][10] social phobia,[11] anxiety,[12] and other conditions.
Surgical procedure
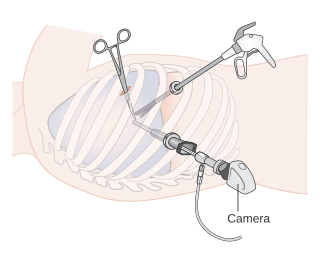
A custom made operating thoracoscope, used for the endoscopic thoracic sympathectomy procedure.
ETS involves dissection of the main sympathetic trunk in the upper thoracic region of the sympathetic nervous system, irreparably disrupting neural messages that ordinarily would travel to many different organs, glands and muscles. It is via those nerves that the brain is able to make adjustments to the body in response to changing conditions in the environment, fluctuating emotional states, level of exercise, and other factors to maintain the body in its ideal state (see homeostasis).
Because these nerves also regulate conditions like excessive blushing or sweating, which the procedure is designed to eliminate, the normative functions these physiological mechanisms perform will be disabled or significantly impaired by sympathectomy.[citation needed]
There is much disagreement among ETS surgeons about the best surgical method, optimal location for nerve dissection, and the nature and extent of the consequent primary effects and side effects. When performed endoscopically as is usually the case, the surgeon penetrates the chest cavity making multiple incisions about the diameter of a straw between ribs. This allows the surgeon to insert the video camera (endoscope) in one hole and a surgical instrument in another. The operation is accomplished by dissecting the nerve tissue of the main sympathetic chain.[citation needed]
Another technique, the clamping method, also referred to as 'endoscopic sympathetic blockade' (ESB) employs titanium clamps around the nerve tissue, and was developed as an alternative to older methods in an unsuccessful attempt to make the procedure reversible. Technical reversal of the clamping procedure must be performed within a short time after clamping (estimated at a few days or weeks at most), and a recovery, evidence indicates, will not be complete.
Physical, mental and emotional effects
Sympathectomy works by disabling part of the autonomic nervous system (and thereby disrupting its signals from the brain), through surgical intervention, in the expectation of removing or alleviating the designated problem. Many non-ETS doctors have found this practice questionable chiefly because its purpose is to destroy functionally disordered, yet anatomically typical nerves.[13]
Exact results of ETS are impossible to predict, because of considerable anatomic variation in nerve function from one patient to the next, and also because of variations in surgical technique. The autonomic nervous system is not anatomically exact and connections might exist which are unpredictably affected when the nerves are disabled. This problem was demonstrated by a significant number of patients who underwent sympathectomy at the same level for hand sweating, but who then presented a reduction or elimination of feet sweating, in contrast to others who were not affected in this way. No reliable operation exists for foot sweating except lumbar sympathectomy, at the opposite end of the sympathetic chain.
A large study of psychiatric patients treated with this surgery showed significant reductions in fear, alertness and arousal.[22] Arousal is essential to consciousness, in regulating attention and information processing, memory and emotion.[23]
ETS patients are being studied using the autonomic failure protocol headed by David Goldstein, M.D. Ph.D., senior investigator at the U.S National Institute of Neurological Disorders and Stroke. He has documented loss of thermoregulatory function, cardiac denervation, and loss of vasoconstriction.[24] Recurrence of the original symptoms due to nerve regeneration or nerve sprouting can occur within the first year post surgery. Nerve sprouting, or abnormal nerve growth after damage or injury to the nerves can cause other further damage. Sprouting sympathetic nerves can form connections with sensory nerves, and lead to pain conditions that are mediated by the SNS. Every time the system is activated, it is translated into pain. This sprouting and its action can lead to Frey's syndrome, a recognized after effect of sympathectomy, when the growing sympathetic nerves innervate salivary glands, leading to excessive sweating regardless of environmental temperature through olfactory or gustatory stimulation.
In addition, patients have reported lethargy, depression, weakness, limb swelling, lack of libido, decreased physical and mental reactivity, oversensitivity to sound, light and stress and weight gain (British Journal of Surgery 2004; 91: 264–269).
Risks
ETS has both the normal risks of surgery, such as bleeding and infection, conversion to open chest surgery, and several specific risks, including permanent and unavoidable alteration of nerve function. It is reported that a number of patients - 9 since 2010, mostly young women - have died during this procedure due to major intrathoracic bleeding and cerebral disruption. Bleeding during and following the operation may be significant in up to 5% of patients.[25]Pneumothorax (collapsed lung) can occur (2% of patients).[25]Compensatory hyperhidrosis (or reflex hyperhidrosis) is common over the long term.[25] The rates of severe compensatory sweating vary widely between studies, ranging from as high as 92% of patients.[26] Of those patients that develop this side effect, about a quarter in one study said it was a major and disabling problem.[27] 35% of people affected have to change their clothes several times a day as a result.[28]
A severe possible consequence of thoracic sympathectomy is corposcindosis (split-body syndrome), in which the patient feels that they are living in two separate bodies, because sympathetic nerve function has been divided into two distinct regions, one dead, and the other hyperactive.[29][medical citation needed]
Additionally, the following side effects have all been reported by patients: Chronic muscular pain, numbness and weakness of the limbs, Horner's Syndrome, anhidrosis (inability to sweat), hyperthermia (exacerbated by anhidrosis and systemic thermoregulatory dysfunction), neuralgia, paraesthesia, fatigue and amotivationality, breathing difficulties, substantially diminished physiological/chemical reaction to internal and environmental stimuli, somatosensory malfunction, aberrant physiological reaction to stress and exertion, Raynaud’s disease (albeit a possible indication for surgery), reflex hyperhidrosis, altered/erratic blood pressure and circulation, defective fight or flight response system, loss of adrenaline, eczema and other skin conditions resulting from exceptionally dry skin, rhinitis, gustatory sweating (also known as Frey's syndrome).[1]
A thermal image of an ETS patient 2 years after surgery.
Other long-term adverse effects include:
Ultrastructural changes in the cerebral artery wall induced by long-term sympathetic denervation[30]
Sympathectomy eliminates the psychogalvanic reflex[31]
Cervical sympathectomy reduces the heterogeneity of oxygen saturation in small cerebrocortical veins[32]
Sympathetic denervation is one of the causes of Mönckeberg's sclerosis[33]
T2-3 sympathectomy suppressed baroreflex control of heart rate in the patients with palmar hyperhidrosis. The baroreflex response for maintaining cardiovascular stability is suppressed in the patients who received the ETS.[19]
Morphofunctional changes in the myocardium following sympathectomy.[34]
Other side effects are the inability to raise the heart rate sufficiently during exercise with instances requiring an artificial pacemaker after developing bradycardia being reported as a consequence of the surgery.[30][35][36]
The Finnish Office for Health Care Technology Assessment concluded more than a decade ago in a 400-page systematic review that ETS is associated with an unusually high number of significant immediate and long-term adverse effects.[37]
Quoting the Swedish National Board of Health and Welfare statement: "The method can give permanent side effects that in some cases will first become obvious only after some time. One of the side effects might be increased perspiration on different places on your body. Why and how this happens is still unknown. According to the research available about 25-75% of all patients can expect more or less serious perspiration on different places on their body, such as the trunk and groin area, this is Compensatory sweating".[38]
In 2003, ETS was banned in its birthplace, Sweden, due to inherent risks, and complaints by disabled patients. In 2004, Taiwanese health authorities banned the procedure on people under 20 years of age.[39]
History
Sympathectomy developed in the mid-19th century, when it was learned that the autonomic nervous system runs to almost every organ, gland and muscle system in the body. It was surmised that these nerves play a role in how the body regulates many different body functions in response to changes in the external environment, and in emotion.[citation needed]
The first sympathectomy was performed by Alexander in 1889.[40] Thoracic sympathectomy has been indicated for hyperhidrosis (excessive sweating) since 1920, when Kotzareff showed it would cause anhidrosis (total inability to sweat) from the nipple line upwards.[14]
A lumbar sympathectomy was also developed and used to treat excessive sweating of the feet and other ailments, and typically resulted in impotence and retrograde ejaculation in men. Lumbar sympathectomy is still being offered as a treatment for plantar hyperhidrosis, or as a treatment for patients who have a bad outcome (extreme 'compensatory sweating') after thoracic sympathectomy for palmar hyperhidrosis or blushing; however, extensive sympathectomy risks hypotension.
Endoscopic sympathectomy itself is relatively easy to perform; however, accessing the nerve tissue in the chest cavity by conventional surgical methods was difficult, painful, and spawned several different approaches in the past. The posterior approach was developed in 1908, and required resection (sawing off) of ribs. A supraclavicular (above the collar-bone) approach was developed in 1935, which was less painful than the posterior, but was more prone to damaging delicate nerves and blood vessels. Because of these difficulties, and because of disabling sequelae associated with sympathetic denervation, conventional or "open" sympathectomy was never a popular procedure, although it continued to be practiced for hyperhidrosis, Raynaud's disease, and various psychiatric disorders. With the brief popularization of lobotomy in the 1940s, sympathectomy fell out of favor as a form of psychosurgery.
The endoscopic version of thoracic sympathectomy was pioneered by Goren Claes and Christer Drott in Sweden in the late 1980s. The development of endoscopic "minimally invasive" surgical techniques has decreased the recovery time from the surgery and increased its availability. Today, ETS surgery is practiced in many countries throughout the world predominantly by vascular surgeons.
Complex regional pain syndrome is a severe form of chronic pain, in which pain from a physical trauma outlasts the expected recovery time. The symptoms of types 1 and 2 are the same except type 2 is associated with nerve injury.
Perspiration, also known as sweat, is the fluid secreted by sweat glands in the skin of mammals.
Dysautonomia, autonomic failure, or autonomic dysfunction is a condition in which the autonomic nervous system (ANS) does not work properly. This may affect the functioning of the heart, bladder, intestines, sweat glands, pupils, and blood vessels. Dysautonomia has many causes, not all of which may be classified as neuropathic. A number of conditions can feature dysautonomia, such as Parkinson's disease, multiple system atrophy, dementia with Lewy bodies, Ehlers–Danlos syndromes, autoimmune autonomic ganglionopathy and autonomic neuropathy, HIV/AIDS, mitochondrial cytopathy, pure autonomic failure, autism, and postural orthostatic tachycardia syndrome.
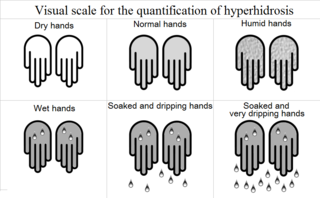
Hyperhidrosis is a medical condition in which a person exhibits excessive sweating, more than that required for the regulation of body temperature. Although it is primarily a physical burden, hyperhidrosis can deteriorate the quality of life of the people who are affected from a psychological, emotional, and social perspective. In fact, hyperhidrosis almost always leads to psychological as well as physical and social consequences. People suffering from it present difficulties in professional fields, more than 80% experiencing a moderate to severe emotional impact from the disease and half are subject to depression.
A sympathectomy is an irreversible procedure during which at least one sympathetic ganglion is removed. One example is the lumbar sympathectomy, which is advised for occlusive arterial disease in which L2 and L3 ganglia along with intervening sympathetic trunk are removed leaving behind the L1 ganglion which is responsible for ejaculation. Another example is endoscopic thoracic sympathectomy.
The baroreflex or baroreceptor reflex is one of the body's homeostatic mechanisms that helps to maintain blood pressure at nearly constant levels. The baroreflex provides a rapid negative feedback loop in which an elevated blood pressure causes the heart rate to decrease. Decreased blood pressure decreases baroreflex activation and causes heart rate to increase and to restore blood pressure levels. Their function is to sense pressure changes by responding to change in the tension of the arterial wall. The baroreflex can begin to act in less than the duration of a cardiac cycle and thus baroreflex adjustments are key factors in dealing with postural hypotension, the tendency for blood pressure to decrease on standing due to gravity.
Horner's syndrome, also known as oculosympathetic paresis, is a combination of symptoms that arises when a group of nerves known as the sympathetic trunk is damaged. The signs and symptoms occur on the same side (ipsilateral) as it is a lesion of the sympathetic trunk. It is characterized by miosis, partial ptosis, apparent anhidrosis, with apparent enophthalmos.
Idiopathic craniofacial erythema is a medical condition characterized by uncontrollable and frequently unprovoked facial blushing.
The stellate ganglion is a sympathetic ganglion formed by the fusion of the inferior cervical ganglion and the first thoracic ganglion, which is present in 80% of individuals. Sometimes, the second and the third thoracic ganglia are included in this fusion.
Harlequin syndrome is a condition characterized by asymmetric sweating and flushing on the upper thoracic region of the chest, neck and face. Harlequin syndrome is considered an injury to the autonomic nervous system (ANS). The ANS controls some of the body's natural processes such as sweating, skin flushing and pupil response to stimuli. Individuals with this syndrome have an absence of sweat skin flushing unilaterally, usually on one side of the face, arms and chest. It is an autonomic disorder that may occur at any age. Harlequin syndrome affects fewer than 1000 people in the United States.
Adie syndrome, also known as Holmes–Adie syndrome, is a neurological disorder characterized by a tonically dilated pupil that reacts slowly to light but shows a more definite response to accommodation. It is frequently seen in females with absent knee or ankle jerks and impaired sweating.
Compensatory hyperhidrosis is a form of neuropathy. It is encountered in patients with myelopathy, thoracic disease, cerebrovascular disease, nerve trauma or after surgeries. The exact mechanism of the phenomenon is poorly understood. It is attributed to the perception in the hypothalamus (brain) that the body temperature is too high. The sweating is induced to reduce body heat.
The lateral grey column is one of the three grey columns of the spinal cord ; the others being the anterior and posterior grey columns. The lateral grey column is primarily involved with activity in the sympathetic division of the autonomic motor system. It projects to the side as a triangular field in the thoracic and upper lumbar regions of the postero-lateral part of the anterior grey column.
A neurectomy, or nerve resection is a neurosurgical procedure in which a peripheral nerve is cut or removed to alleviate neuropathic pain or permanently disable some function of a nerve. The nerve is not intended to grow back. For chronic pain it may be an alternative to a failed nerve decompression when the target nerve has no motor function and numbness is acceptable. Neurectomies have also been used to permanently block autonomic function, and special sensory function not related to pain.
Frey's syndrome is a rare neurological disorder resulting from damage to or near the parotid glands responsible for making saliva, and from damage to the auriculotemporal nerve often from surgery.
Video-assisted thoracoscopic surgery (VATS) is a type of minimally invasive thoracic surgery performed using a small video camera mounted to a fiberoptic thoracoscope, with or without angulated visualization, which allows the surgeon to see inside the chest by viewing the video images relayed onto a television screen, and perform procedures using elongated surgical instruments. The camera and instruments are inserted into the patient's chest cavity through small incisions in the chest wall, usually via specially designed guiding tubes known as "ports".
Denervation is any loss of nerve supply regardless of the cause. If the nerves lost to denervation are part of the neuronal communication to a specific function in the body then altered or a loss of physiological functioning can occur. Denervation can be caused by injury or be a symptom of a disorder like ALS, post-polio syndrome, or POTS. Additionally, it can be a useful surgical technique to alleviate major negative symptoms, such as in renal denervation. Denervation can have many harmful side effects such as increased risk of infection and tissue dysfunction.
Palmoplantar hyperhidrosis is excessive sweating localized to the palms of the hands and soles of the feet. It is a form of focal hyperhidrosis in that the excessive sweating is limited to a specific region of the body. As with other types of focal hyperhidrosis the sweating tends to worsen during warm weather.
Focal hyperhidrosis, also known as primary hyperhidrosis, is a disease characterized by an excessive sweating localized in certain body regions. Studies suggest that this condition, affecting between 1% and 3% of the US population, seems to have a genetic predisposition in about two thirds of those affected.
Carpal tunnel surgery, also called carpal tunnel release (CTR) and carpal tunnel decompression surgery, is a nerve decompression in which the transverse carpal ligament is divided. It is a surgical treatment for carpal tunnel syndrome (CTS) and recommended when there is constant (not just intermittent) numbness, muscle weakness, or atrophy, and when night-splinting no longer controls intermittent symptoms of pain in the carpal tunnel. In general, milder cases can be controlled for months to years, but severe cases are unrelenting symptomatically and are likely to result in surgical treatment. Approximately 500,000 surgical procedures are performed each year, and the economic impact of this condition is estimated to exceed $2 billion annually.
↑ Miranda-Sivelo A, Bajo-Del Pozo C, Fructuoso-Castellar A (2013). "Unnecessary surgical treatment in a case of olfactory reference syndrome". General Hospital Psychiatry. 35 (6): 683.e3–4. doi:10.1016/j.genhosppsych.2013.06.014. PMID23992627.
↑ Suzuki J, Takaku A, Kodama N, Sato S (1975). "An Attempt to Treat Cerebrovascular 'Moyamoya' Disease in Children". Pediatric Neurosurgery. 1 (4): 193–206. doi:10.1159/000119568. PMID1183260.
↑ Pohjavaara P, Telaranta T, Väisänen E (2003). "The role of the sympathetic nervous system in anxiety: Is it possible to relieve anxiety with endoscopic sympathetic block?". Nordic Journal of Psychiatry. 57 (1): 55–60. doi:10.1080/08039480310000266. PMID12745792. S2CID28944767.
↑ Milner P, Lincoln J, Burnstock G (1998). "The neurochemical organization of the autonomic nervous system". In Appenzeller O, Vinken PJ, Bruyn GW (eds.). The autonomic nervous system. [Amsterdam, Netherlands]: Elsevier Science Publishers. pp.110. ISBN0-444-82812-5.
↑ Bassenge E, Holtz J, von Restorff W, Oversohl K (July 1973). "Effect of chemical sympathectomy on coronary flow and cardiovascular adjustment to exercise in dogs". Pflügers Archiv. 341 (4): 285–96. doi:10.1007/BF01023670. PMID4798744. S2CID20076364.
↑ Furlan AD, Mailis A, Papagapiou M (2000). "Are We Paying a High Price for Surgical Sympathectomy? A Systematic Literature Review of Late Complications". The Journal of Pain. 1 (4): 245–57. doi:10.1054/jpai.2000.19408. PMID14622605.
↑ Beskrovnova NN, Makarychev VA, Kiseleva ZM, Legon'kaia, Zhuchkova NI (1984). "Morphofunctional changes in the myocardium following sympathectomy and their role in the development of sudden death from ventricular fibrillation". Vestnik Akademii Meditsinskikh Nauk SSSR (2): 80–5. PMID6711115.
↑ Lai CL, Chen WJ, Liu YB, Lee YT (2001). "Bradycardia and Permanent Pacing After Bilateral Thoracoscopic T2-Sympathectomy for Primary Hyperhidrosis". Pacing and Clinical Electrophysiology. 24 (4): 524–5. doi:10.1046/j.1460-9592.2001.00524.x. PMID11341096. S2CID13586588.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.