
The larynx, commonly called the voice box, is an organ in the top of the neck involved in breathing, producing sound and protecting the trachea against food aspiration. The opening of larynx into pharynx known as the laryngeal inlet is about 4–5 centimeters in diameter. The larynx houses the vocal cords, and manipulates pitch and volume, which is essential for phonation. It is situated just below where the tract of the pharynx splits into the trachea and the esophagus. The word 'larynx' comes from the Ancient Greek word lárunx ʻlarynx, gullet, throatʼ.

The trachea, also known as the windpipe, is a cartilaginous tube that connects the larynx to the bronchi of the lungs, allowing the passage of air, and so is present in almost all animals lungs. The trachea extends from the larynx and branches into the two primary bronchi. At the top of the trachea, the cricoid cartilage attaches it to the larynx. The trachea is formed by a number of horseshoe-shaped rings, joined together vertically by overlying ligaments, and by the trachealis muscle at their ends. The epiglottis closes the opening to the larynx during swallowing.

Tracheal intubation, usually simply referred to as intubation, is the placement of a flexible plastic tube into the trachea (windpipe) to maintain an open airway or to serve as a conduit through which to administer certain drugs. It is frequently performed in critically injured, ill, or anesthetized patients to facilitate ventilation of the lungs, including mechanical ventilation, and to prevent the possibility of asphyxiation or airway obstruction.
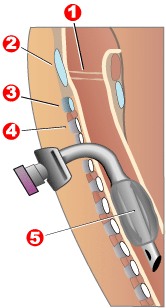
Tracheotomy, or tracheostomy, is a surgical airway management procedure which consists of making an incision (cut) on the anterior aspect (front) of the neck and opening a direct airway through an incision in the trachea (windpipe). The resulting stoma (hole) can serve independently as an airway or as a site for a tracheal tube or tracheostomy tube to be inserted; this tube allows a person to breathe without the use of the nose or mouth.

Laryngoscopy is endoscopy of the larynx, a part of the throat. It is a medical procedure that is used to obtain a view, for example, of the vocal folds and the glottis. Laryngoscopy may be performed to facilitate tracheal intubation during general anaesthesia or cardiopulmonary resuscitation or for surgical procedures on the larynx or other parts of the upper tracheobronchial tree.

Laryngectomy is the removal of the larynx. In a total laryngectomy, the entire larynx is removed with the separation of the airway from the mouth, nose and esophagus. In a partial laryngectomy, only a portion of the larynx is removed. Following the procedure, the person breathes through an opening in the neck known as a stoma. This procedure is usually performed by an ENT surgeon in cases of laryngeal cancer. Many cases of laryngeal cancer are treated with more conservative methods. A laryngectomy is performed when these treatments fail to conserve the larynx or when the cancer has progressed such that normal functioning would be prevented. Laryngectomies are also performed on individuals with other types of head and neck cancer. Less invasive partial laryngectomies, including tracheal shaves and feminization laryngoplasty may also be performed on transgender women and other female or non-binary identified individuals to feminize the larynx and/or voice. Post-laryngectomy rehabilitation includes voice restoration, oral feeding and more recently, smell and taste rehabilitation. An individual's quality of life can be affected post-surgery.

The recurrent laryngeal nerve (RLN) is a branch of the vagus nerve that supplies all the intrinsic muscles of the larynx, with the exception of the cricothyroid muscles. There are two recurrent laryngeal nerves, right and left. The right and left nerves are not symmetrical, with the left nerve looping under the aortic arch, and the right nerve looping under the right subclavian artery, then traveling upwards. They both travel alongside the trachea. Additionally, the nerves are among the few nerves that follow a recurrent course, moving in the opposite direction to the nerve they branch from, a fact from which they gain their name.

The posterior cricoarytenoid muscle is a intrinsic muscle of the larynx. It arises from the cricoid cartilage; it inserts onto the arytenoid cartilage of the same side. It is innervated by the recurrent laryngeal nerve. Each acts to open the vocal folds by pulling the vocal fold of the same side laterally. It participates in the production of sounds.

The cricoid cartilage, or simply cricoid or cricoid ring, is the only complete ring of cartilage around the trachea. It forms the back part of the voice box and functions as an attachment site for muscles, cartilages, and ligaments involved in opening and closing the airway and in producing speech.
Chondrolaryngoplasty is a surgical procedure in which the thyroid cartilage is reduced in size by shaving down the cartilage through an incision in the throat, generally to aid those who are uncomfortable with the girth of their Adam's apple.

The arytenoid cartilages are a pair of small three-sided pyramids which form part of the larynx. They are the site of attachment of the vocal cords. Each is pyramidal or ladle-shaped and has three surfaces, a base, and an apex. The arytenoid cartilages allow for movement of the vocal cords by articulating with the cricoid cartilage. They may be affected by arthritis, dislocations, or sclerosis.

Laryngomalacia is the most common cause of chronic stridor in infancy, in which the soft, immature cartilage of the upper larynx collapses inward during inhalation, causing obstruction of the airways. It can also be seen in older patients, especially those with neuromuscular conditions resulting in weakness of the muscles of the throat. However, the infantile form is much more common. Laryngomalacia is one of the most common laryngeal congenital diseases in infancy and public education about the signs and symptoms of the disease is lacking.
Subglottic stenosis is a congenital or acquired narrowing of the subglottic airway. It can be congenital, acquired, iatrogenic, or very rarely, idiopathic. It is defined as the narrowing of the portion of the airway that lies between the vocal cords and the lower part of the cricoid cartilage. In a normal infant, the subglottic airway is 4.5-5.5 millimeters wide, while in a premature infant, the normal width is 3.5 millimeters. Subglottic stenosis is defined as a diameter of under 4 millimeters in an infant. Acquired cases are more common than congenital cases due to prolonged intubation being introduced in the 1960s. It is most frequently caused by certain medical procedures or external trauma, although infections and systemic diseases can also cause it.

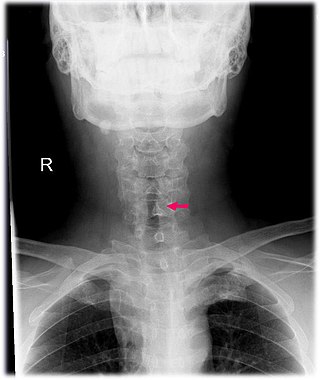
Laryngotracheal stenosis refers to abnormal narrowing of the central air passageways. This can occur at the level of the larynx, trachea, carina or main bronchi. In a small number of patients narrowing may be present in more than one anatomical location.
A cricoidectomy is the surgical excision of the cricoid cartilage. The excision can often be performed under local anaesthetic and can either be partial or total. The procedure may be necessary as a treatment of pulmonary aspiration, to prevent progression to aspiration pneumonia. As the cricoid cartilage is the narrowest part of the trachea, it is also a common point of a blockage or narrowing (stenosis).
A laryngeal cleft or laryngotracheoesophageal cleft is a rare congenital abnormality in the posterior laryngo-tracheal wall. It occurs in approximately 1 in 10,000 to 20,000 births. It means there is a communication between the oesophagus and the trachea, which allows food or fluid to pass into the airway.
Laryngeal cysts are cysts involving the larynx or more frequently supraglottic locations, such as epiglottis and vallecula. Usually they do not extend to the thyroid cartilage. They may be present congenitally or may develop eventually due to degenerative cause. They often interfere with phonation.
Endoscopic laser cordectomy, also known as Kashima operation, is an endoscopic laser surgical procedure performed for treating the respiratory difficulty caused as a result of bilateral abductor vocal fold paralysis. Bilateral vocal fold paralysis is basically a result of abnormal nerve input to the laryngeal muscles, resulting in weak or total loss of movement of the laryngeal muscles. Most commonly associated nerve is the vagus nerve or in some cases its distal branch, the recurrent laryngeal nerve. Paralysis of the vocal fold may also result from mechanical breakdown of the cricoarytenoid joint. It was first described in by Kashima in 1989.
Arytenoid adduction is a surgical procedure used to treat vocal cord paralysis. A suture is used to emulate the action of the lateral cricoarytenoid muscle and position the paralyzed vocal cord closer to the midline. This allows the two vocal cords to meet and can improve speaking and swallowing ability for affected patients. Arytenoid adduction is often performed in conjunction with medialization thyroplasty.

Intubation granuloma is a benign growth of granulation tissue in the larynx or trachea, which arises from tissue trauma due to endotracheal intubation. This medical condition is described as a common late complication of tracheal intubation, specifically caused by irritation to the mucosal tissue of the airway during insertion or removal of the patient's intubation tube.