
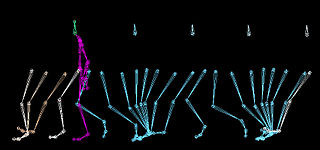
Running is a method of terrestrial locomotion by which humans and other animals move rapidly on foot. Running is a gait with an aerial phase in which all feet are above the ground. This is in contrast to walking, where one foot is always in contact with the ground, the legs are kept mostly straight, and the center of gravity vaults over the stance leg or legs in an inverted pendulum fashion. A feature of a running body from the viewpoint of spring-mass mechanics is that changes in kinetic and potential energy within a stride co-occur, with energy storage accomplished by springy tendons and passive muscle elasticity. The term "running" can refer to a variety of speeds ranging from jogging to sprinting.
Walking is one of the main gaits of terrestrial locomotion among legged animals. Walking is typically slower than running and other gaits. Walking is defined by an "inverted pendulum" gait in which the body vaults over the stiff limb or limbs with each step. This applies regardless of the usable number of limbs—even arthropods, with six, eight, or more limbs, walk. In humans, walking has health benefits including improved mental health and reduced risk of cardiovascular disease and death.

Leptin, also known as obese protein, is a protein hormone predominantly made by adipocytes. Its primary role is likely to regulate long-term energy balance.

Adipose tissue is a loose connective tissue composed mostly of adipocytes. It also contains the stromal vascular fraction (SVF) of cells including preadipocytes, fibroblasts, vascular endothelial cells and a variety of immune cells such as adipose tissue macrophages. Its main role is to store energy in the form of lipids, although it also cushions and insulates the body.

A gait is a manner of limb movements made during locomotion. Human gaits are the various ways in which humans can move, either naturally or as a result of specialized training. Human gait is defined as bipedal forward propulsion of the center of gravity of the human body, in which there are sinuous movements of different segments of the body with little energy spent. Various gaits are characterized by differences in limb movement patterns, overall velocity, forces, kinetic and potential energy cycles, and changes in contact with the ground.

Weight gain is an increase in body weight. This can involve an increase in muscle mass, fat deposits, excess fluids such as water or other factors. Weight gain can be a symptom of a serious medical condition.
Bariatrics is a discipline that deals with the causes, prevention, and treatment of obesity, encompassing both obesity medicine and bariatric surgery.
Running economy (RE) a complex, multifactorial concept that represents the sum of metabolic, cardiorespiratory, biomechanical and neuromuscular efficiency during running. Oxygen consumption (VO2) is the most commonly used method for measuring running economy, as the exchange of gases in the body, specifically oxygen and carbon dioxide, closely reflects energy metabolism. Those who are able to consume less oxygen while running at a given velocity are said to have a better running economy. However, straightforward oxygen usage does not account for whether the body is metabolising lipids or carbohydrates, which produce different amounts of energy per unit of oxygen; as such, accurate measurements of running economy must use O2 and CO2 data to estimate the calorific content of the substrate that the oxygen is being used to respire.
Adipose tissue is an endocrine organ that secretes numerous protein hormones, including leptin, adiponectin, and resistin. These hormones generally influence energy metabolism, which is of great interest to the understanding and treatment of type 2 diabetes and obesity.

Being overweight is having more body fat than is optimally healthy. Being overweight is especially common where food supplies are plentiful and lifestyles are sedentary.
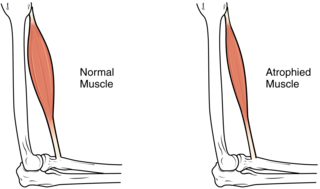
Sarcopenic obesity is a combination of two disease states, sarcopenia and obesity. Sarcopenia is the muscle mass/strength/physical function loss associated with increased age, and obesity is based off a weight to height ratio or body mass index (BMI) that is characterized by high body fat or being overweight.
Running energetics is the study of the energy cost of running. It is clear in the vast majority of species that as running speed increases the energetic cost of running increases. It also has long been known that between and within species variability exists in the energy cost of running a given speed. This variability has led to the study of biomechanical or physiological factors that may be predictive of the energy cost to run both between and within species.
The preferred walking speed is the speed at which humans or animals choose to walk. Many people tend to walk at about 1.42 metres per second. Individuals may find slower or faster speeds uncomfortable.
Human locomotion is considered to take two primary forms: walking and running. In contrast, many quadrupeds have three distinct forms of locomotion: walk, trot, and gallop. Walking is a form of locomotion defined by a double support phase when both feet are on the ground at the same time. Running is a form of locomotion that does not have this double support phase.
Terrestrial locomotion by means of a running gait can be accomplished on level surfaces. However, in most outdoor environments an individual will experience terrain undulations requiring uphill running. Similar conditions can be mimicked in a controlled environment on a treadmill also. Additionally, running on inclines is used by runners, both distance and sprinter, to improve cardiovascular conditioning and lower limb strength.
Neuromechanics of orthoses refers to how the human body interacts with orthoses. Millions of people in the U.S. suffer from stroke, multiple sclerosis, postpolio, spinal cord injuries, or various other ailments that benefit from the use of orthoses. Insofar as active orthoses and powered exoskeletons are concerned, the technology to build these devices is improving rapidly, but little research has been done on the human side of these human-machine interfaces.

The effect of gait parameters on energetic cost is a relationship that describes how changes in step length, cadence, step width, and step variability influence the mechanical work and metabolic cost involved in gait. The source of this relationship stems from the deviation of these gait parameters from metabolically optimal values, with the deviations due to environmental, pathological, and other factors.
Normal weight obesity is the condition of having normal body weight, but with a high body fat percentage, leading to some of the same health risks as obesity.

Gait deviations are nominally referred to as any variation of standard human gait, typically manifesting as a coping mechanism in response to an anatomical impairment. Lower-limb amputees are unable to maintain the characteristic walking patterns of an able-bodied individual due to the removal of some portion of the impaired leg. Without the anatomical structure and neuromechanical control of the removed leg segment, amputees must use alternative compensatory strategies to walk efficiently. Prosthetic limbs provide support to the user and more advanced models attempt to mimic the function of the missing anatomy, including biomechanically controlled ankle and knee joints. However, amputees still display quantifiable differences in many measures of ambulation when compared to able-bodied individuals. Several common observations are whole-body movements, slower and wider steps, shorter strides, and increased sway.
Energy expenditure, often estimated as the total daily energy expenditure (TDEE), is the amount of energy burned by the human body.