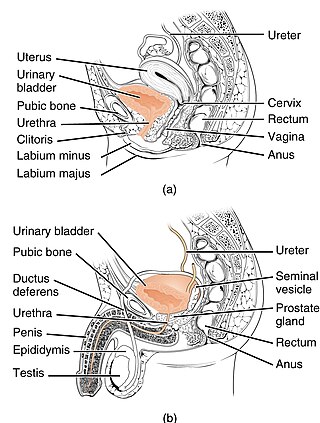
The urethra is a tube that connects the urinary bladder to the urinary meatus for the removal of urine from the body of both female and male mammals. In female humans and other primates, the urethra connects to the urinary meatus above the vagina.

The pudendal nerve is the main nerve of the perineum. It is a mixed nerve and also conveys sympathetic autonomic fibers. It carries sensation from the external genitalia of both sexes and the skin around the anus and perineum, as well as the motor supply to various pelvic muscles, including the male or female external urethral sphincter and the external anal sphincter.

Urination is the release of urine from the bladder through the urethra to the outside of the body. It is the urinary system's form of excretion. It is also known medically as micturition, voiding, uresis, or, rarely, emiction, and known colloquially by various names including peeing, weeing, pissing, and euphemistically going number one. In healthy humans and other animals, the process of urination is under voluntary control. In infants, some elderly individuals, and those with neurological injury, urination may occur as a reflex. It is normal for adult humans to urinate up to seven times during the day.
Urinary incontinence (UI), also known as involuntary urination, is any uncontrolled leakage of urine. It is a common and distressing problem, which may have a large impact on quality of life. It has been identified as an important issue in geriatric health care. The term enuresis is often used to refer to urinary incontinence primarily in children, such as nocturnal enuresis. UI is an example of a stigmatized medical condition, which creates barriers to successful management and makes the problem worse. People may be too embarrassed to seek medical help, and attempt to self-manage the symptom in secrecy from others.

The parasympathetic nervous system (PSNS) is one of the three divisions of the autonomic nervous system, the others being the sympathetic nervous system and the enteric nervous system. The enteric nervous system is sometimes considered part of the autonomic nervous system, and sometimes considered an independent system.
Articles related to anatomy include:

The external sphincter muscle of male urethra, also sphincter urethrae membranaceae, sphincter urethrae externus, surrounds the whole length of the membranous urethra, and is enclosed in the fascia of the urogenital diaphragm.

Bladder sphincter dyssynergia is a consequence of a neurological pathology such as spinal injury or multiple sclerosis which disrupts central nervous system regulation of the micturition (urination) reflex resulting in dyscoordination of the detrusor muscles of the bladder and the male or female external urethral sphincter muscles. In normal lower urinary tract function, these two separate muscle structures act in synergistic coordination. But in this neurogenic disorder, the urethral sphincter muscle, instead of relaxing completely during voiding, dyssynergically contracts causing the flow to be interrupted and the bladder pressure to rise.
Neurogenic bladder dysfunction, often called by the shortened term neurogenic bladder, refers to urinary bladder problems due to disease or injury of the central nervous system or peripheral nerves involved in the control of urination. There are multiple types of neurogenic bladder depending on the underlying cause and the symptoms. Symptoms include overactive bladder, urinary urgency, frequency, incontinence or difficulty passing urine. A range of diseases or conditions can cause neurogenic bladder including spinal cord injury, multiple sclerosis, stroke, brain injury, spina bifida, peripheral nerve damage, Parkinson's disease, or other neurodegenerative diseases. Neurogenic bladder can be diagnosed through a history and physical as well as imaging and more specialized testing. In addition to symptomatic treatment, treatment depends on the nature of the underlying disease and can be managed with behavioral changes, medications, surgeries, or other procedures. The symptoms of neurogenic bladder, especially incontinence, can severely degrade a person's quality of life.
A sacral anterior root stimulator is an implantable medical device enabling patients with a spinal cord lesion to empty their bladders.

The urethral sphincters are two muscles used to control the exit of urine in the urinary bladder through the urethra. The two muscles are either the male or female external urethral sphincter and the internal urethral sphincter. When either of these muscles contracts, the urethra is sealed shut.

The internal urethral sphincter is a urethral sphincter muscle which constricts the internal urethral orifice. It is located at the junction of the urethra with the urinary bladder and is continuous with the detrusor muscle, but anatomically and functionally fully independent from it. It is composed of smooth muscle, so it is under the control of the autonomic nervous system, specifically the sympathetic nervous system.
Sacral nerve stimulation, also termed sacral neuromodulation, is a type of medical electrical stimulation therapy.

The external sphincter muscle of female urethra is a muscle which controls urination in females. The muscle fibers arise on either side from the margin of the inferior ramus of the pubis. They are directed across the pubic arch in front of the urethra, and pass around it to blend with the muscular fibers of the opposite side, between the urethra and vagina.
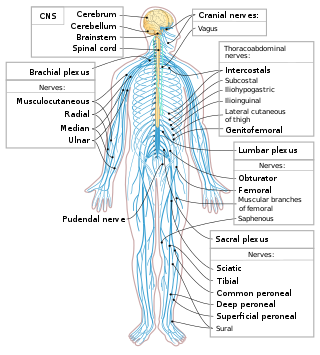
The spinal cord is a long, thin, tubular structure made up of nervous tissue that extends from the medulla oblongata in the brainstem to the lumbar region of the vertebral column (backbone) of vertebrate animals. The center of the spinal cord is hollow and contains a structure called central canal, which contains cerebrospinal fluid. The spinal cord is also covered by meninges and enclosed by the neural arches. Together, the brain and spinal cord make up the central nervous system.
The pontine micturition center is a collection of neuronal cell bodies located in the rostral pons in the brainstem involved in the supraspinal regulation of micturition. When activated, the PMC relaxes the urethral sphincter allowing for micturition to occur. The PMC coordinates with other brain centers, including the medial frontal cortex, insular cortex, hypothalamus and periaqueductal gray (PAG). The PAG acts as a relay station for ascending bladder information from the spinal cord and incoming signals from higher brain areas.

Overflow incontinence is a concept of urinary incontinence, characterized by the involuntary release of urine from an overfull urinary bladder, often in the absence of any urge to urinate. This condition occurs in people who have a blockage of the bladder outlet, or when the muscle that expels urine from the bladder is too weak to empty the bladder normally. Overflow incontinence may also be a side effect of certain medications.
Dyssynergia is any disturbance of muscular coordination, resulting in uncoordinated and abrupt movements. This is also an aspect of ataxia. It is typical for dyssynergic patients to split a movement into several smaller movements. Types of dyssynergia include Ramsay Hunt syndrome type 1, bladder sphincter dyssynergia, and anal sphincter dyssynergia.

A lumbar anterior root stimulator is a type of neuroprosthesis used in patients with a spinal cord injury or to treat some forms of chronic spinal pain. More specifically, the root stimulator can be used in patients who have lost proper bowel function due to damaged neurons related to gastrointestinal control and potentially allow paraplegics to exercise otherwise paralyzed leg muscles.

Neurogenic bowel dysfunction (NBD) is the inability to control defecation due to a deterioration of or injury to the nervous system, resulting in faecal incontinence or constipation. It is common in people with spinal cord injury (SCI), multiple sclerosis (MS) or spina bifida.
