Skin cancers are cancers that arise from the skin. They are due to the development of abnormal cells that have the ability to invade or spread to other parts of the body. There are three main types of skin cancers: basal-cell skin cancer (BCC), squamous-cell skin cancer (SCC) and melanoma. The first two, along with a number of less common skin cancers, are known as nonmelanoma skin cancer (NMSC). Basal-cell cancer grows slowly and can damage the tissue around it but is unlikely to spread to distant areas or result in death. It often appears as a painless raised area of skin that may be shiny with small blood vessels running over it or may present as a raised area with an ulcer. Squamous-cell skin cancer is more likely to spread. It usually presents as a hard lump with a scaly top but may also form an ulcer. Melanomas are the most aggressive. Signs include a mole that has changed in size, shape, color, has irregular edges, has more than one color, is itchy or bleeds.

Thyroid neoplasm is a neoplasm or tumor of the thyroid. It can be a benign tumor such as thyroid adenoma, or it can be a malignant neoplasm, such as papillary, follicular, medullary or anaplastic thyroid cancer. Most patients are 25 to 65 years of age when first diagnosed; women are more affected than men. The estimated number of new cases of thyroid cancer in the United States in 2010 is 44,670 compared to only 1,690 deaths. Of all thyroid nodules discovered, only about 5 percent are cancerous, and under 3 percent of those result in fatalities.
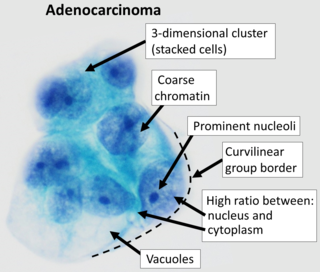
Adenocarcinoma (AC) is a type of cancerous tumor that can occur in several parts of the body. It is defined as neoplasia of epithelial tissue that has glandular origin, glandular characteristics, or both. Adenocarcinomas are part of the larger grouping of carcinomas, but are also sometimes called by more precise terms omitting the word, where these exist. Thus invasive ductal carcinoma, the most common form of breast cancer, is adenocarcinoma but does not use the term in its name—however, esophageal adenocarcinoma does to distinguish it from the other common type of esophageal cancer, esophageal squamous cell carcinoma. Several of the most common forms of cancer are adenocarcinomas, and the various sorts of adenocarcinoma vary greatly in all their aspects, so that few useful generalizations can be made about them.
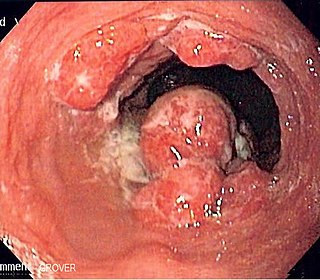
Esophageal cancer is cancer arising from the esophagus—the food pipe that runs between the throat and the stomach. Symptoms often include difficulty in swallowing and weight loss. Other symptoms may include pain when swallowing, a hoarse voice, enlarged lymph nodes ("glands") around the collarbone, a dry cough, and possibly coughing up or vomiting blood.

Carcinoma is a malignancy that develops from epithelial cells. Specifically, a carcinoma is a cancer that begins in a tissue that lines the inner or outer surfaces of the body, and that arises from cells originating in the endodermal, mesodermal or ectodermal germ layer during embryogenesis.

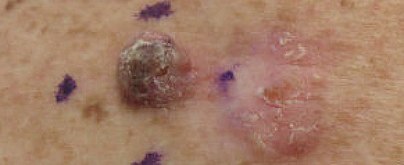
Cutaneous squamous-cell carcinoma (cSCC), also known as squamous-cell skin cancer, is one of the main types of skin cancer along with basal-cell carcinoma and melanoma. It usually presents as a hard lump with a scaly top but can also form an ulcer. Onset is often over months. Cutaneous squamous-cell carcinoma is more likely to spread to distant areas than basal cell cancer. When confined to the outermost layer of the skin, a precancerous or in situ form of cSCC is known as Bowen's disease.

Head and neck cancer develops from tissues in the lip and oral cavity (mouth), larynx (throat), salivary glands, nose, sinuses or the skin of the face. The most common types of head and neck cancers occur in the lip, mouth, and larynx. Symptoms predominantly include a sore that does not heal or a change in the voice. Some may experience a sore throat that does not go away. In those with advanced disease, there may be unusual bleeding, facial pain, numbness or swelling, and visible lumps on the outside of the neck or oral cavity. Given the location of these cancers, trouble breathing may also be present.
Gastrointestinal cancer refers to malignant conditions of the gastrointestinal tract and accessory organs of digestion, including the esophagus, stomach, biliary system, pancreas, small intestine, large intestine, rectum and anus. The symptoms relate to the organ affected and can include obstruction, abnormal bleeding or other associated problems. The diagnosis often requires endoscopy, followed by biopsy of suspicious tissue. The treatment depends on the location of the tumor, as well as the type of cancer cell and whether it has invaded other tissues or spread elsewhere. These factors also determine the prognosis.
Non-small-cell lung cancer (NSCLC), or non-small-cell lung carcinoma, is any type of epithelial lung cancer other than small-cell lung cancer (SCLC). NSCLC accounts for about 85% of all lung cancers. As a class, NSCLCs are relatively insensitive to chemotherapy, compared to small-cell carcinoma. When possible, they are primarily treated by surgical resection with curative intent, although chemotherapy has been used increasingly both preoperatively and postoperatively.

Nasopharyngeal carcinoma (NPC), or nasopharynx cancer, is the most common cancer originating in the nasopharynx, most commonly in the postero-lateral nasopharynx or pharyngeal recess, accounting for 50% of cases. NPC occurs in children and adults. NPC differs significantly from other cancers of the head and neck in its occurrence, causes, clinical behavior, and treatment. It is vastly more common in certain regions of East Asia and Africa than elsewhere, with viral, dietary and genetic factors implicated in its causation. It is most common in males. It is a squamous cell carcinoma of an undifferentiated type. Squamous epithelial cells are a flat type of cell found in the skin and the membranes that line some body cavities. Undifferentiated cells are cells that do not have their mature features or functions.
The International Cancer Genome Consortium (ICGC) is a voluntary scientific organization that provides a forum for collaboration among the world's leading cancer and genomic researchers. The ICGC was launched in 2008 to coordinate large-scale cancer genome studies in tumours from 50 cancer types and/or subtypes that are of main importance across the globe.
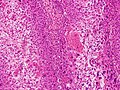
Large cell lung carcinoma with rhabdoid phenotype (LCLC-RP) is a rare histological form of lung cancer, currently classified as a variant of large cell lung carcinoma (LCLC). In order for a LCLC to be subclassified as the rhabdoid phenotype variant, at least 10% of the malignant tumor cells must contain distinctive structures composed of tangled intermediate filaments that displace the cell nucleus outward toward the cell membrane. The whorled eosinophilic inclusions in LCLC-RP cells give it a microscopic resemblance to malignant cells found in rhabdomyosarcoma (RMS), a rare neoplasm arising from transformed skeletal muscle. Despite their microscopic similarities, LCLC-RP is not associated with rhabdomyosarcoma.
Salivary gland–like carcinomas of the lung generally refers a class of rare cancers that arise from the uncontrolled cell division (mitosis) of mutated cancer stem cells in lung tissue. They take their name partly from the appearance of their abnormal cells, whose structure and features closely resemble those of cancers that form in the major salivary glands of the head and neck. Carcinoma is a term for malignant neoplasms derived from cells of epithelial lineage, and/or that exhibit cytological or tissue architectural features characteristically found in epithelial cells.
Skin cancer, or neoplasia, is the most common type of cancer diagnosed in horses, accounting for 45 to 80% of all cancers diagnosed. Sarcoids are the most common type of skin neoplasm and are the most common type of cancer overall in horses. Squamous-cell carcinoma is the second-most prevalent skin cancer, followed by melanoma. Squamous-cell carcinoma and melanoma usually occur in horses greater than 9-years-old, while sarcoids commonly affect horses 3 to 6 years old. Surgical biopsy is the method of choice for diagnosis of most equine skin cancers, but is contraindicated for cases of sarcoids. Prognosis and treatment effectiveness varies based on type of cancer, degree of local tissue destruction, evidence of spread to other organs (metastasis) and location of the tumor. Not all cancers metastasize and some can be cured or mitigated by surgical removal of the cancerous tissue or through use of chemotherapeutic drugs.

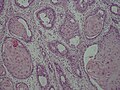
Ceruminous adenocarcinoma is a malignant neoplasm derived from ceruminous glands of the external auditory canal. This tumor is rare, with several names used in the past. Synonyms have included cylindroma, ceruminoma, ceruminous adenocarcinoma, not otherwise specified (NOS), ceruminous adenoid cystic carcinoma (ACC), and ceruminous mucoepidermoid carcinoma.
Conjunctival squamous cell carcinoma and corneal intraepithelial neoplasia comprise what are called ocular surface squamous cell neoplasias. SCC is the most common malignancy of the conjunctiva in the US, with a yearly incidence of 1–2.8 per 100,000. Risk factors for the disease are exposure to sun, exposure to UVB, and light-colored skin. Other risk factors include radiation, smoking, HPV, arsenic, and exposure to polycyclic hydrocarbons.

Oesophagogastric junctional adenocarcinoma is a cancer of the lower part of the oesophagus with a rising incidence in Western countries. This disease is often linked to Barrett's oesophagus.

Squamous-cell carcinoma (SCC) of the lung is a histologic type of non-small-cell lung carcinoma (NSCLC). It is the second most prevalent type of lung cancer after lung adenocarcinoma and it originates in the bronchi. Its tumor cells are characterized by a squamous appearance, similar to the one observed in epidermal cells. Squamous-cell carcinoma of the lung is strongly associated with tobacco smoking, more than any other forms of NSCLC.

Bartholin gland carcinoma is a type of cancer of the vulva arising in the Bartholin gland. It typically presents with a painless mass at one side of the vaginal opening in a female of middle-age and older, and can appear similar to a Bartholin cyst. The mass may be big or small, may be deep under skin or appear nearer the surface with overlying ulceration. Average age at presentation is 53-years.