
Thyroid neoplasm is a neoplasm or tumor of the thyroid. It can be a benign tumor such as thyroid adenoma, or it can be a malignant neoplasm, such as papillary, follicular, medullary or anaplastic thyroid cancer. Most patients are 25 to 65 years of age when first diagnosed; women are more affected than men. The estimated number of new cases of thyroid cancer in the United States in 2010 is 44,670 compared to only 1,690 deaths. Of all thyroid nodules discovered, only about 5 percent are cancerous, and under 3 percent of those result in fatalities.

Carcinoma is a category of types of cancer that develop from epithelial cells. Specifically, a carcinoma is a cancer that begins in a tissue that lines the inner or outer surfaces of the body, and that arises from cells originating in the endodermal, mesodermal or ectodermal germ layer during embryogenesis.

Surface epithelial-stromal tumors are a class of ovarian neoplasms that may be benign or malignant. Neoplasms in this group are thought to be derived from the ovarian surface epithelium or from ectopic endometrial or Fallopian tube (tubal) tissue. Tumors of this type are also called ovarian adenocarcinoma. This group of tumors accounts for 90% to 95% of all cases of ovarian cancer. Serum CA-125 is often elevated but is only 50% accurate so it is not a useful tumor marker to assess the progress of treatment.
The International Classification of Diseases for Oncology (ICD-O) is a domain-specific extension of the International Statistical Classification of Diseases and Related Health Problems for tumor diseases. This classification is widely used by cancer registries.

A Hürthle cell is a cell in the thyroid that is often associated with Hashimoto's thyroiditis as well as benign and malignant tumors. This version is a relatively rare form of differentiated thyroid cancer, accounting for only 3-10% of all differentiated thyroid cancers. Oncocytes in the thyroid are often called Hürthle cells. Although the terms oncocyte, oxyphilic cell, and Hürthle cell are used interchangeably, Hürthle cell is used only to indicate cells of thyroid follicular origin.
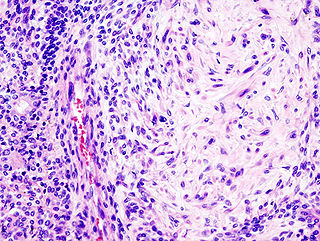
Pleomorphic adenoma is a common benign salivary gland neoplasm characterised by neoplastic proliferation of parenchymatous glandular cells along with myoepithelial components, having a malignant potentiality. It is the most common type of salivary gland tumor and the most common tumor of the parotid gland. It derives its name from the architectural Pleomorphism seen by light microscopy. It is also known as "Mixed tumor, salivary gland type", which refers to its dual origin from epithelial and myoepithelial elements as opposed to its pleomorphic appearance.

Anaplastic thyroid cancer (ATC), also known as anaplastic thyroid carcinoma, is an aggressive form of thyroid cancer characterized by uncontrolled growth of cells in the thyroid gland. This form of cancer generally carries a very poor prognosis due to its aggressive behavior and resistance to cancer treatments. The cells of anaplastic thyroid cancer are highly abnormal and usually no longer resemble the original thyroid cells and have poor differentiation.

Papillary thyroid cancer or papillary thyroid carcinoma is the most common type of thyroid cancer, representing 75 percent to 85 percent of all thyroid cancer cases. It occurs more frequently in women and presents in the 20–55 year age group. It is also the predominant cancer type in children with thyroid cancer, and in patients with thyroid cancer who have had previous radiation to the head and neck. It is often well-differentiated, slow-growing, and localized, although it can metastasize.
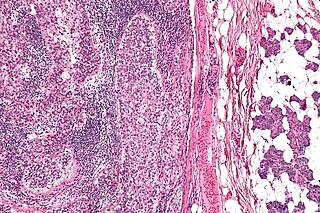
An adrenal tumor or adrenal mass is any benign or malignant neoplasms of the adrenal gland, several of which are notable for their tendency to overproduce endocrine hormones. Adrenal cancer is the presence of malignant adrenal tumors, and includes neuroblastoma, adrenocortical carcinoma and some adrenal pheochromocytomas. Most adrenal pheochromocytomas and all adrenocortical adenomas are benign tumors, which do not metastasize or invade nearby tissues, but may cause significant health problems by unbalancing hormones.
Metaplastic carcinoma, otherwise known as metaplastic carcinoma of the breast (MCB), is a heterogeneous group of cancers that exhibit varied patterns of metaplasia and differentiation along multiple cell lines. This rare and aggressive form of breast cancer is characterized as being composed of a mixed group of neoplasms containing both glandular and non-glandular patterns with epithelial and/or mesenchymal components. It accounts for fewer than 1% of all breast cancer diagnoses. It is most closely associated with invasive ductal carcinoma of no special type. (IDC), and shares similar treatment approaches. Relative to IDC, MCB generally has higher histological grade and larger tumor size at time of diagnoses, but a lower incidence of axillary lymph node involvement. MCB tumors are typically estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor-2 (HER-2) negative, meaning hormone therapy is generally not an effective treatment option, which correlates to a relatively poor prognosis. MCB was first recognized as a distinct pathological entity in 2000 by the World Health Organization.

Salivary gland tumours or neoplasms are tumours that form in the tissues of salivary glands. The salivary glands are classified as major or minor. The major salivary glands consist of the parotid, submandibular, and sublingual glands. The minor salivary glands consist of 800-1000 small mucus-secreting glands located throughout the lining of the oral cavity.
ICD-10 is an international statistical classification used in health care and related industries.
Sebaceous carcinoma, also known as sebaceous gland carcinoma (SGc), sebaceous cell carcinoma, and mebomian gland carcinoma is an uncommon and aggressive malignant cutaneous tumor. Most are typically about 10 mm in size at presentation. This neoplasm is thought to arise from sebaceous glands in the skin and, therefore, may originate anywhere in the body where these glands are found. Sebaceous carcinoma can be divided into 2 types: ocular and extraocular. Because the periocular region is rich in this type of gland, this region is a common site of origin. The cause of these lesions are, in the vast majority of cases, unknown. Occasional cases may be associated with Muir-Torre syndrome. Due to the rarity of this tumor and variability in clinical and histological presentation, SGc is often misdiagnosed as an inflammatory condition or a more common type of tumor.
Large cell lung carcinoma with rhabdoid phenotype (LCLC-RP) is a rare histological form of lung cancer, currently classified as a variant of large cell lung carcinoma (LCLC). In order for a LCLC to be subclassified as the rhabdoid phenotype variant, at least 10% of the malignant tumor cells must contain distinctive structures composed of tangled intermediate filaments that displace the cell nucleus outward toward the cell membrane. The whorled eosinophilic inclusions in LCLC-RP cells give it a microscopic resemblance to malignant cells found in rhabdomyosarcoma (RMS), a rare neoplasm arising from transformed skeletal muscle. Despite their microscopic similarities, LCLC-RP is not associated with rhabdomyosarcoma.
Giant-cell carcinoma of the lung (GCCL) is a rare histological form of large-cell lung carcinoma, a subtype of undifferentiated lung cancer, traditionally classified within the non-small-cell lung carcinomas (NSCLC).
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) is an indolent thyroid tumor that was previously classified as an encapsulated follicular variant of papillary thyroid carcinoma, necessitating a new classification as it was recognized that encapsulated tumors without invasion have an indolent behavior, and may be over-treated if classified as a type of cancer.

Bartholin gland carcinoma is an uncommon type of malignancy in the Bartholin gland that accounts for 1% of all vulvar malignant neoplasms. It is most common in women in their mid-60s. The tumor can become large before a woman is aware of symptoms. One of the first symptoms can be dyspareunia. In other instances a woman may find a mass or ulcer in the vulva area. Many clinicians assume that an enlarged Bartholin gland is malignant in postmenopausal woman until proven otherwise. The growth of the tumor can spread to nearby areas such as the ischiorectal fossa and inguinal lymph nodes. Approximately 50% of bartholin gland carcinomas originate from squamous cell carcinomas. Another uncommon characteristic of Bartholin gland malignancies is that the growth of a lesion originates from the three types of epithelial tissue present in the gland: mucinous, transitional, and squamous.
Squamous cell carcinomas (SCCs), also known as epidermoid carcinomas, comprise a number of different types of cancer that result from squamous cells. These cells form on the surface of the skin, on the lining of hollow organs in the body, and on the lining of the respiratory and digestive tracts.
In CT scan of the thyroid, focal and diffuse thyroid abnormalities are commonly encountered. These findings can often lead to a diagnostic dilemma, as the CT reflects the nonspecific appearances. Ultrasound (US) examination has a superior spatial resolution and is considered the modality of choice for thyroid evaluation. Nevertheless, CT detects incidental thyroid nodules (ITNs) and plays an important role in the evaluation of thyroid cancer.
