Related Research Articles
Optic neuritis describes any condition that causes inflammation of the optic nerve; it may be associated with demyelinating diseases, or infectious or inflammatory processes.

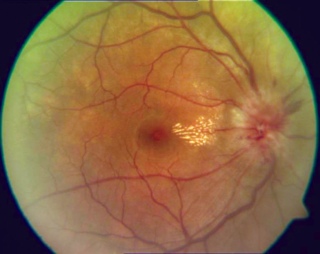
The retina is the innermost, light-sensitive layer of tissue of the eye of most vertebrates and some molluscs. The optics of the eye create a focused two-dimensional image of the visual world on the retina, which then processes that image within the retina and sends nerve impulses along the optic nerve to the visual cortex to create visual perception. The retina serves a function which is in many ways analogous to that of the film or image sensor in a camera.

Ophthalmology is a surgical subspecialty within medicine that deals with the diagnosis and treatment of eye disorders. A former term is oculism.

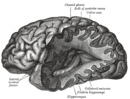
In neuroanatomy, the optic nerve, also known as the second cranial nerve, cranial nerve II, or simply CN II, is a paired cranial nerve that transmits visual information from the retina to the brain. In humans, the optic nerve is derived from optic stalks during the seventh week of development and is composed of retinal ganglion cell axons and glial cells; it extends from the optic disc to the optic chiasma and continues as the optic tract to the lateral geniculate nucleus, pretectal nuclei, and superior colliculus.

Papilledema or papilloedema is optic disc swelling that is caused by increased intracranial pressure due to any cause. The swelling is usually bilateral and can occur over a period of hours to weeks. Unilateral presentation is extremely rare.

Retinitis pigmentosa (RP) is a genetic disorder of the eyes that causes loss of vision. Symptoms include trouble seeing at night and decreasing peripheral vision. As peripheral vision worsens, people may experience "tunnel vision". Complete blindness is uncommon. Onset of symptoms is generally gradual and often begins in childhood.
The National Eye Institute (NEI) is part of the U.S. National Institutes of Health (NIH), an agency of the U.S. Department of Health and Human Services. The mission of NEI is "to eliminate vision loss and improve quality of life through vision research." NEI consists of two major branches for research: an extramural branch that funds studies outside NIH and an intramural branch that funds research on the NIH campus in Bethesda, Maryland. Most of the NEI budget funds extramural research.
Photophobia is a medical symptom of abnormal intolerance to visual perception of light. As a medical symptom, photophobia is not a morbid fear or phobia, but an experience of discomfort or pain to the eyes due to light exposure or by presence of actual physical sensitivity of the eyes, though the term is sometimes additionally applied to abnormal or irrational fear of light, such as heliophobia. The term photophobia comes from the Greek φῶς (phōs), meaning "light", and φόβος (phóbos), meaning "fear".
The visual field is "that portion of space in which objects are visible at the same moment during steady fixation of the gaze in one direction"; in ophthalmology and neurology the emphasis is on the structure inside the visual field and it is then considered “the field of functional capacity obtained and recorded by means of perimetry”.

Diplopia is the simultaneous perception of two images of a single object that may be displaced horizontally or vertically in relation to each other. Also called double vision, it is a loss of visual focus under regular conditions, and is often voluntary. However, when occurring involuntarily, it results in impaired function of the extraocular muscles, where both eyes are still functional, but they cannot turn to target the desired object. Problems with these muscles may be due to mechanical problems, disorders of the neuromuscular junction, disorders of the cranial nerves that innervate the muscles, and occasionally disorders involving the supranuclear oculomotor pathways or ingestion of toxins.

The optic disc or optic nerve head is the point of exit for ganglion cell axons leaving the eye. Because there are no rods or cones overlying the optic disc, it corresponds to a small blind spot in each eye.

Leber's hereditary optic neuropathy (LHON) is a mitochondrially inherited degeneration of retinal ganglion cells (RGCs) and their axons that leads to an acute or subacute loss of central vision; it predominantly affects young adult males. LHON is transmitted only through the mother, as it is primarily due to mutations in the mitochondrial genome, and only the egg contributes mitochondria to the embryo. Men cannot pass on the disease to their offspring. LHON is usually due to one of three pathogenic mitochondrial DNA (mtDNA) point mutations. These mutations are at nucleotide positions 11778 G to A, 3460 G to A and 14484 T to C, respectively in the ND4, ND1 and ND6 subunit genes of complex I of the oxidative phosphorylation chain in mitochondria.
Anterior ischemic optic neuropathy (AION) is a medical condition involving loss of vision caused by damage to the optic nerve as a result of insufficient blood supply (ischemia). This form of ischemic optic neuropathy is generally categorized as two types: arteritic AION, in which the loss of vision is the result of an inflammatory disease of arteries in the head called temporal arteritis, and non-arteritic AION, which is due to non-inflammatory disease of small blood vessels.
Dominant optic atrophy (DOA), or autosomal dominant optic atrophy (ADOA), (Kjer's type) is an autosomally inherited disease that affects the optic nerves, causing reduced visual acuity and blindness beginning in childhood. However, the disease can seem to re-present a second time with further vision loss due to the early onset of presbyopia symptoms (i.e., difficulty in viewing objects up close). DOA is characterized as affecting neurons called retinal ganglion cells (RGCs). This condition is due to mitochondrial dysfunction mediating the death of optic nerve fibers. The RGCs axons form the optic nerve. Therefore, the disease can be considered of the central nervous system. Dominant optic atrophy was first described clinically by Batten in 1896 and named Kjer’s optic neuropathy in 1959 after Danish ophthalmologist Poul Kjer, who studied 19 families with the disease. Although dominant optic atrophy is the most common autosomally inherited optic neuropathy (i.e., disease of the optic nerves), it is often misdiagnosed.
Optic neuropathy is damage to the optic nerve from any cause. The optic nerve is a bundle of millions of fibers in the retina that sends visual signals to the brain. [1].

Optic disc drusen (ODD) are globules of mucoproteins and mucopolysaccharides that progressively calcify in the optic disc. They are thought to be the remnants of the axonal transport system of degenerated retinal ganglion cells. ODD have also been referred to as congenitally elevated or anomalous discs, pseudopapilledema, pseudoneuritis, buried disc drusen, and disc hyaline bodies.

Bonnet–Dechaume–Blanc syndrome, also known as Wyburn-Mason syndrome, is a rare congenital disorder characterized by arteriovenous malformations of the brain, retina or facial nevi. The syndrome has a number of possible symptoms and can, more rarely, affect the skin, bones, kidneys, muscles, and gastrointestinal tract. When the syndrome affects the brain, people can experience severe headaches, seizures, acute stroke, meningism, and progressive neurological deficits due to acute or chronic ischaemia caused by arteriovenous shunting.
Mitohondrial optic neuropathies are a heterogenous group of disorders that present with visual disturbances resultant from mitochondrial dysfunction within the anatomy of the Retinal Ganglion Cells (RGC), optic nerve, optic chiasm, and optic tract. These disturbances are multifactorial, their aetiology consisting of metabolic and/or structural damage as a consequence of genetic mutations, environmental stressors, or both. The three most common neuro-ophthalmic abnormalities seen in mitochondrial disorders are bilateral optic neuropathy, ophthalmoplegia with ptosis, and pigmentary retinopathy.
Chronic relapsing inflammatory optic neuropathy (CRION) is a form of recurrent optic neuritis that is steroid responsive and dependent. Patients typically present with pain associated with visual loss. CRION is a clinical diagnosis of exclusion, and other demyelinating, autoimmune, and systemic causes should be ruled out. An accurate antibody test which became available commercially in 2017 has allowed most patients previously diagnosed with CRION to be re-identified as having MOG antibody disease, which is not a diagnosis of exclusion. Early recognition is crucial given risks for severe visual loss and because it is treatable with immunosuppressive treatment such as steroids or B-cell depleting therapy. Relapse that occurs after reducing or stopping steroids is a characteristic feature.

Alfredo Arrigo Sadun is an American ophthalmologist, academic, author and researcher. He holds the Flora L. Thornton Endowed Chair at Doheny Eye Centers-UCLA and is Vice-Chair of Ophthalmology at UCLA.
References
- 1 2 Lessell, S (Apr 2000). "What can we expect in neuro-ophthalmology in the next century?". Archives of Ophthalmology. 118 (4): 553–4. doi: 10.1001/archopht.118.4.553 . PMID 10766142.
- ↑ "North American Neuro-Ophthalmology Society". North American Neuro-Ophthalmology Society Home Page. Archived from the original on 26 September 2014. Retrieved 28 September 2014.
- ↑ McDonnell, Peter (1 Nov 2004). "Is neuro-ophthalmology in jeopardy?". Ophthalmology Times. 29 (21): 4. Archived from the original on 2 April 2015.
- ↑ Frohman, LP (Sep 2008). "The human resource crisis in neuro-ophthalmology". Journal of Neuro-Ophthalmology. 28 (3): 231–4. doi: 10.1097/wno.0b013e318185e084 . PMID 18769291.
- ↑ Spitze, A; Al-Zubidi, N; Lam, P; Yalamanchili, S; Lee, AG (October 2014). "Neuro-ophthalmology as a career". Indian Journal of Ophthalmology. 62 (10): 1013–4. doi: 10.4103/0301-4738.146007 . PMC 4278112 . PMID 25449937.
- ↑ Posey, William Campbell; Spiller, William G. (1906). The Eye and Nervous System: Their Diagnostic Relations by Various Authors. Philadelphia and London: J.B. Lippincott Company.
- ↑ Angelucci, Diane. "Groundbreaking neuro-ophthalmologist honored". EyeWorld. Archived from the original on 5 March 2015. Retrieved 28 September 2014.
- ↑ Newman, SA (Jun 2012). "Interventional neuro-ophthalmology: not an oxymoron". Journal of Neuro-Ophthalmology. 32 (2): 177–84. doi: 10.1097/wno.0b013e318256638e . PMID 22617746. S2CID 35672897.
- ↑ Lam, BL; Feuer, WJ; Schiffman, JC; Porciatti, V; Vandenbroucke, R; Rosa, PR; Gregori, G; Guy, J (Apr 1, 2014). "Trial end points and natural history in patients with G11778A Leber hereditary optic neuropathy : preparation for gene therapy clinical trial". JAMA Ophthalmology. 132 (4): 428–36. doi:10.1001/jamaophthalmol.2013.7971. PMC 4266137 . PMID 24525545.
- ↑ Watanabe, M; Fukuda, Y (Nov 2002). "Survival and axonal regeneration of retinal ganglion cells in adult cats". Progress in Retinal and Eye Research. 21 (6): 529–53. doi:10.1016/s1350-9462(02)00037-x. PMID 12433376. S2CID 46211858.
- ↑ Xia, Y; Nawy, S; Carroll, RC (Nov 7, 2007). "Activity-dependent synaptic plasticity in retinal ganglion cells". The Journal of Neuroscience. 27 (45): 12221–9. doi:10.1523/jneurosci.2086-07.2007. PMC 3073613 . PMID 17989288.
- ↑ "NEI Audacious Goal Initiative". National Eye Institute. Retrieved 28 September 2014.