Lars Leksell (1907–1986) was a Swedish physician and Professor of Neurosurgery at the Karolinska Institute in Stockholm, Sweden. He was the inventor of radiosurgery.

Radiosurgery is surgery using radiation, that is, the destruction of precisely selected areas of tissue using ionizing radiation rather than excision with a blade. Like other forms of radiation therapy, it is usually used to treat cancer. Radiosurgery was originally defined by the Swedish neurosurgeon Lars Leksell as "a single high dose fraction of radiation, stereotactically directed to an intracranial region of interest".

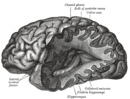
Stereotactic surgery is a minimally invasive form of surgical intervention that makes use of a three-dimensional coordinate system to locate small targets inside the body and to perform on them some action such as ablation, biopsy, lesion, injection, stimulation, implantation, radiosurgery (SRS), etc.
Image-guided surgery (IGS) is any surgical procedure where the surgeon uses tracked surgical instruments in conjunction with preoperative or intraoperative images in order to directly or indirectly guide the procedure. Image guided surgery systems use cameras, ultrasonic, electromagnetic or a combination of fields to capture and relay the patient's anatomy and the surgeon's precise movements in relation to the patient, to computer monitors in the operating room or to augmented reality headsets. This is generally performed in real-time though there may be delays of seconds or minutes depending on the modality and application.
The study of neurology and neurosurgery dates back to prehistoric times, but the academic disciplines did not begin until the 16th century. From an observational science they developed a systematic way of approaching the nervous system and possible interventions in neurological disease.
Brain biopsy is the removal of a small piece of brain tissue for the diagnosis of abnormalities of the brain. It is used to diagnose tumors, infection, inflammation, and other brain disorders. By examining the tissue sample under a microscope, the biopsy sample provides information about the appropriate diagnosis and treatment.
Hypophysectomy is the surgical removal of the hypophysis. It is most commonly performed to treat tumors, especially craniopharyngioma tumors. Sometimes it is used to treat Cushing's syndrome due to pituitary adenoma or Simmond's disease It is also applied in neurosciences to understand the functioning of hypophysis. There are various ways a hypophysectomy can be carried out. These methods include transsphenoidal hypophysectomy, open craniotomy, and stereotactic radiosurgery.
The Neurologic & Orthopedic Hospital of Chicago was a medical center from 1987 to 2009.
Ablative brain surgery is the surgical ablation by various methods of brain tissue to treat neurological or psychological disorders. The word "Ablation" stems from the Latin word Ablatus meaning "carried away". In most cases, however, ablative brain surgery does not involve removing brain tissue, but rather destroying tissue and leaving it in place. The lesions it causes are irreversible. There are some target nuclei for ablative surgery and deep brain stimulation. Those nuclei are the motor thalamus, the globus pallidus, and the subthalamic nucleus.
Neurosurgical anesthesiology, neuroanesthesiology, or neurological anesthesiology is a subspecialty of anesthesiology devoted to the total perioperative care of patients before, during, and after neurological surgeries, including surgeries of the central (CNS) and peripheral nervous systems (PNS). The field has undergone extensive development since the 1960s correlating with the ability to measure intracranial pressure (ICP), cerebral blood flow (CBF), and cerebral metabolic rate (CMR).
Roger Härtl is an American neurological surgeon at Weill-Cornell Medical College and NewYork-Presbyterian Hospital. He is the Director of Spinal Surgery at the Weill Cornell Brain & Spine Center. Härtl has been named by Becker's Spine Review as one of the Top 50 Spine Surgeons in the United States as well as one of the Top 10 Spine and Neurosurgeon Leaders at Non-Profit Hospitals. He was named one of New York's Top Doctors by New York Magazine after he saved the life of New York firefighter Eugene Stolowski.

Michael L. J. Apuzzo is an American academic neurological surgeon, the Edwin M. Todd/Trent H. Wells, Jr. Professor Emeritus of Neurological Surgery and Radiation Oncology, Biology, and Physics at the Keck School of Medicine, of the University of Southern California. He is also editor emeritus of the peer-reviewed journals World Neurosurgery and Neurosurgery. He is distinguished adjunct professor of neurosurgery at the Yale School of Medicine, distinguished professor of advanced neurosurgery and neuroscience and senior advisor, at the Neurological Institute, Wexner Medical School, The Ohio State University, and adjunct professor of neurosurgery, Weill Cornell Medicine, Department of Neurological Surgery & Weill Cornell Brain and Spine Center.
Minimally invasive spine surgery, also known as MISS, has no specific meaning or definition. It implies a lack of severe surgical invasion. The older style of open-spine surgery for a relatively small disc problem used to require a 5-6 inch incision and a month in the hospital. MISS techniques utilize more modern technology, advanced imaging techniques and special medical equipment to reduce tissue trauma, bleeding, radiation exposure, infection risk, and decreased hospital stays by minimizing the size of the incision. Modern endoscopic procedures can be done through a 2 to 5 mm skin opening. By contrast, procedures done with a microscope require skin openings of approximately one inch, or more.

Aaron A. Cohen-Gadol is a professor of neurological surgery in the department of neurosurgery at Indiana University School of Medicine and a neurosurgeon at Indiana University Health specializing in the surgical treatment of complex brain tumors, vascular malformations, cavernous malformations, etc. He performs removal of brain tumors via minimally invasive endoscopic techniques, which use the nasal pathways instead of opening the skull.

Jefferson Hospital for Neuroscience is a hospital in Center City Philadelphia, affiliated with Thomas Jefferson University and Thomas Jefferson University Hospital in Philadelphia. The hospital focuses on treating brain-related diseases and disorders. It is the only hospital of its kind in the Philadelphia area.
Nazir Ahmad is a neurosurgeon from Pakistan.
Robert Wheeler Rand, was an American neurosurgeon, inventor, and Professor of Neurosurgery in the Department of Neurosurgery at the University of California Los Angeles (UCLA) from 1953 to 1989.

Dr. Basant Kumar Misra is a neurosurgeon specialising in treating brain, spine, cerebrovascular and peripheral nervous system disorders, injuries, pathologies and malformations. He is the Vice-President of the World Federation of Neurosurgical Societies, and the former President of the Asian Australasian Society of Neurological Surgeons, and the Neurological Society of India. He is a recipient of Dr. B. C. Roy Award, the highest medical honour in India.

Konstantin Slavin is a Professor and Head of the Department of Stereotactic and functional neurosurgery at the University of Illinois College of Medicine. He is a former president of the American Society for Stereotactic and functional neurosurgery and current vice-president of the World Society for Stereotactic and Functional Neurosurgery. His specialties include Aneurysm, Brain surgery, Brain Tumor, Cerebrovascular Disorders, Craniotomy, Dystonia, Essential Tremor, Facial Nerve Pain, Facial Pain, Glioblastoma, Headache disorders, Laminectomy, Lower back pain, Movement Disorders, Multiple Sclerosis, Neck Pain, Neurosurgery, Neurosurgical Procedures, Pain, Parkinson Disease, Spinal Cord Injuries, and Stroke.

Deepak Agrawal born 10 November 1970, is a professor neurosurgery at All India Institute of Medical Sciences, New Delhi is one of the top 10 surgeons in the neurosurgery. During his stint as chairman computarization, he reformed the ICT processes at AIIMS, New Delhi and also helped patients in All India Institute of Medical Sciences, New Delhi to get a Unique Health Identification (UHID), which documents their journey in the hospital. He also pioneered stem cell research in spinal cord injury in India. Agrawal has pioneered DREZotomy technique for neuropathic pain in India and has refined the procedure to make it safer and more accessible to patients.

 A doctor performing Stereotactic Gamma Knife Radiosurgery, a non-invasive procedure
A doctor performing Stereotactic Gamma Knife Radiosurgery, a non-invasive procedure Puma Robotic Arm
Puma Robotic Arm Aluminum headrest
Aluminum headrest