Benign prostatic hyperplasia (BPH), also called prostate enlargement, is a noncancerous increase in size of the prostate gland. Symptoms may include frequent urination, trouble starting to urinate, weak stream, inability to urinate, or loss of bladder control. Complications can include urinary tract infections, bladder stones, and chronic kidney problems.

Beta blockers, also spelled β-blockers, are a class of medications that are predominantly used to manage abnormal heart rhythms (arrhythmia), and to protect the heart from a second heart attack after a first heart attack. They are also widely used to treat high blood pressure, although they are no longer the first choice for initial treatment of most patients.
Atenolol is a beta blocker medication primarily used to treat high blood pressure and heart-associated chest pain. Atenolol, however, does not seem to improve mortality in those with high blood pressure. Other uses include the prevention of migraines and treatment of certain irregular heart beats. It is taken orally or by intravenous injection. It can also be used with other blood pressure medications.
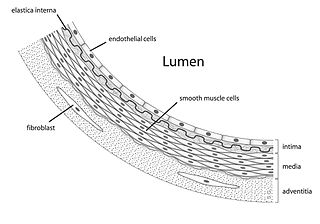
Vascular smooth muscle is the type of smooth muscle that makes up most of the walls of blood vessels.

Doxazosin, sold under the brand names Cardura among others, is a medication used to treat symptoms of benign prostatic hyperplasia and hypertension. For high blood pressure, it is a less preferred option. It is taken by mouth.

Prazosin, sold under the brand name Minipress among others, is a medication used to treat high blood pressure, symptoms of an enlarged prostate, and nightmares related to post-traumatic stress disorder (PTSD). It is an α1 blocker. It is a less preferred treatment of high blood pressure. Other uses may include heart failure and Raynaud syndrome. It is taken by mouth.

Alfuzosin, sold under the brand name Uroxatral among others, is a medication of the α1 blocker class. It is used to treat benign prostatic hyperplasia (BPH).

Phenoxybenzamine is a non-selective, irreversible alpha blocker.
Nocturia is defined by the International Continence Society (ICS) as “the complaint that the individual has to wake at night one or more times for voiding .” The term is derived from Latin nox, night, and Greek [τα] ούρα, urine. Causes are varied and can be difficult to discern. Although not every patient needs treatment, most people seek treatment for severe nocturia, waking up to void more than 2–3 times per night.
Tamsulosin, sold under the brand name Flomax among others, is a medication used to treat symptomatic benign prostatic hyperplasia (BPH) and chronic prostatitis and to help with the passage of kidney stones. The evidence for benefit with a kidney stone is better when the stone is larger. It is taken by mouth.
Moxonidine (INN) is a new-generation alpha-2/imidazoline receptor agonist antihypertensive drug licensed for the treatment of mild to moderate essential hypertension. It may have a role when thiazides, beta-blockers, ACE inhibitors, and calcium channel blockers are not appropriate or have failed to control blood pressure. In addition, it demonstrates favourable effects on parameters of the insulin resistance syndrome, apparently independent of blood pressure reduction. It is also a growth hormone releaser. It is manufactured by Solvay Pharmaceuticals under the brand name Physiotens and Moxon.
Labetalol is a medication used to treat high blood pressure and in long term management of angina. This includes essential hypertension, hypertensive emergencies, and hypertension of pregnancy. In essential hypertension it is generally less preferred than a number of other blood pressure medications. It can be given by mouth or by injection into a vein.
Intraoperative floppy iris syndrome (IFIS) is a complication that may occur during cataract extraction in certain patients. This syndrome is characterized by a flaccid iris which billows in response to ordinary intraocular fluid currents, a propensity for this floppy iris to prolapse towards the area of cataract extraction during surgery, and progressive intraoperative pupil constriction despite standard procedures to prevent this.

Silodosin, sold under the brand name Urief among others, is a medication for the symptomatic treatment of benign prostatic hyperplasia. It acts as an alpha-1 adrenergic receptor antagonist.

An adrenergic antagonist is a drug that inhibits the function of adrenergic receptors. There are five adrenergic receptors, which are divided into two groups. The first group of receptors are the beta (β) adrenergic receptors. There are β1, β2, and β3 receptors. The second group contains the alpha (α) adrenoreceptors. There are only α1 and α2 receptors. Adrenergic receptors are located near the heart, kidneys, lungs, and gastrointestinal tract. There are also α-adreno receptors that are located on vascular smooth muscle.
The first-dose phenomenon is a sudden and severe fall in blood pressure that can occur when changing from a lying to a standing position the first time that an alpha blocker drug is used or when resuming the drug after many months off. This postural hypotension usually happens shortly after the first dose is absorbed into the blood and can result in syncope (fainting). Syncope occurs in approximately 1% of patients given an initial dose of 2 mg prazosin or greater. This adverse effect is self-limiting and in most cases does not recur after the initial period of therapy or during subsequent dose titration.

The alpha-1A adrenergic receptor, also known as ADRA1A, formerly known also as the alpha-1C adrenergic receptor, is an alpha-1 adrenergic receptor, and also denotes the human gene encoding it. There is no longer a subtype α1C receptor. At one time, there was a subtype known as α1C, but it was found to be identical to the previously discovered α1A receptor subtype. To avoid confusion, the naming convention was continued with the letter D.

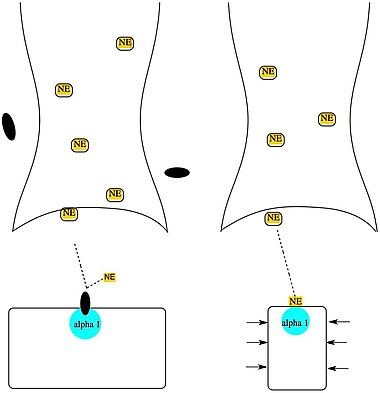
Alpha-blockers, also known as α-blockers or α-adrenoreceptor antagonists, are a class of pharmacological agents that act as antagonists on α-adrenergic receptors (α-adrenoceptors).
Adrenergic blocking agents are a class of drugs that exhibit its pharmacological action through inhibiting the action of the sympathetic nervous system in the body. The sympathetic nervous system(SNS) is an autonomic nervous system that we cannot control by will. It triggers a series of responses after the body releases chemicals named noradrenaline and epinephrine. These chemicals will act on adrenergic receptors, with subtypes Alpha-1, Alpha-2, Beta-1, Beta-2, Beta-3, which ultimately allow the body to trigger a "fight-or-flight" response to handle external stress. These responses include vessel constriction in general vessels whereas there is vasodilation in vessels that supply skeletal muscles or in coronary vessels. Additionally, the heart rate and contractile force increase when SNS is activated, which may be harmful to cardiac function as it increases metabolic demand.
Adrenergic neurone blockers, commonly known as adrenergic antagonists, are a group of drugs that inhibit the sympathetic nervous system by blocking the activity of adrenergic neurones. They prevent the action or release of catecholamines such as norepinephrine and epinephrine. They are located throughout the body, causing various physiological reactions including bronchodilation, accelerated heartbeat, and vasoconstriction. They work by inhibiting the synthesis, release, or reuptake of the neurotransmitters or by antagonising the receptors on postsynaptic neurones. Their medical uses, mechanisms of action, adverse effects, and contraindications depend on the specific types of adrenergic blockers used, including alpha 1, alpha 2, beta 1, and beta 2.