
Cranial nerves are the nerves that emerge directly from the brain, of which there are conventionally considered twelve pairs. Cranial nerves relay information between the brain and parts of the body, primarily to and from regions of the head and neck, including the special senses of vision, taste, smell, and hearing.
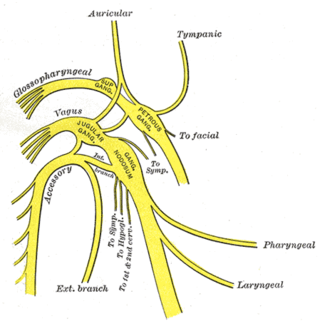
The vagus nerve, also known as the tenth cranial nerve, cranial nerve X, or simply CN X, is a cranial nerve that carries sensory fibers that create a pathway that interfaces with the parasympathetic control of the heart, lungs, and digestive tract. It comprises two nerves—the left and right vagus nerves, each containing about 100,000 fibres—but they are typically referred to collectively as a single subsystem.

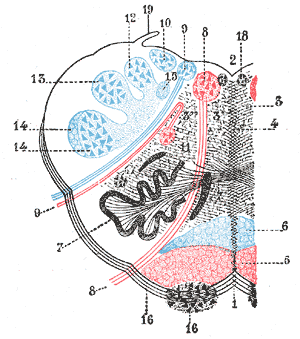
The medulla oblongata or simply medulla is a long stem-like structure which makes up the lower part of the brainstem. It is anterior and partially inferior to the cerebellum. It is a cone-shaped neuronal mass responsible for autonomic (involuntary) functions, ranging from vomiting to sneezing. The medulla contains the cardiac, respiratory, vomiting and vasomotor centers, and therefore deals with the autonomic functions of breathing, heart rate and blood pressure as well as the sleep–wake cycle. "Medulla" is from Latin, ‘pith or marrow’. And "oblongata" is from Latin, ‘lengthened or longish or elongated'.
The brainstem is the stalk-like part of the brain that connects the forebrain with the spinal cord. In the human brain, the brainstem is composed of the midbrain, the pons, and the medulla oblongata. The midbrain is continuous with the thalamus of the diencephalon through the tentorial notch.
The glossopharyngeal nerve, also known as the ninth cranial nerve, cranial nerve IX, or simply CN IX, is a cranial nerve that exits the brainstem from the sides of the upper medulla, just anterior to the vagus nerve. Being a mixed nerve (sensorimotor), it carries afferent sensory and efferent motor information. The motor division of the glossopharyngeal nerve is derived from the basal plate of the embryonic medulla oblongata, whereas the sensory division originates from the cranial neural crest.

The hypoglossal nerve, also known as the twelfth cranial nerve, cranial nerve XII, or simply CN XII, is a cranial nerve that innervates all the extrinsic and intrinsic muscles of the tongue except for the palatoglossus, which is innervated by the vagus nerve. CN XII is a nerve with a sole motor function. The nerve arises from the hypoglossal nucleus in the medulla as a number of small rootlets, pass through the hypoglossal canal and down through the neck, and eventually passes up again over the tongue muscles it supplies into the tongue.

The somatic nervous system (SNS) is made up of nerves that link the brain and spinal cord to voluntary or skeletal muscles that are under conscious control as well as to skin sensory receptors. Specialized nerve fiber ends called sensory receptors are responsible for detecting information within and outside of the body.

The pyramidal tracts include both the corticobulbar tract and the corticospinal tract. These are aggregations of efferent nerve fibers from the upper motor neurons that travel from the cerebral cortex and terminate either in the brainstem (corticobulbar) or spinal cord (corticospinal) and are involved in the control of motor functions of the body.

The solitary nucleus is a series of sensory nuclei forming a vertical column of grey matter in the medulla oblongata of the brainstem. It receives general visceral and/or special visceral inputs from the facial nerve, glossopharyngeal nerve and vagus nerve ; it receives and relays stimuli related to taste and visceral sensation. It sends outputs to various parts of the brain, such as the hypothalamus, thalamus, and reticular formation. Neuron cell bodies of the SN are roughly somatotopically arranged along its length according to function.
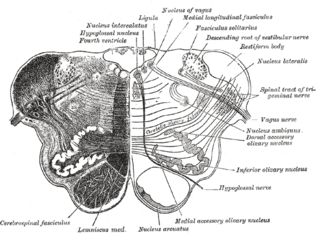
The nucleus ambiguus is a group of large motor neurons situated in the reticular formation of the medulla oblongata of the brainstem. It represents a shared cranial nerve nucleus of the glossopharyngeal nerve, and vagus nerve ; the cranial root of accessory nerve is now also considered as (displaced) fibers of CN X arising from the caudal nucleus ambiguus to travel some distance with those of the CN XI before joining the main CN X.
Medial medullary syndrome, also known as inferior alternating syndrome, hypoglossal alternating hemiplegia, lower alternating hemiplegia, or Dejerine syndrome, is a type of alternating hemiplegia characterized by a set of clinical features resulting from occlusion of the anterior spinal artery. This results in the infarction of medial part of the medulla oblongata.

The fourth ventricle is one of the four connected fluid-filled cavities within the human brain. These cavities, known collectively as the ventricular system, consist of the left and right lateral ventricles, the third ventricle, and the fourth ventricle. The fourth ventricle extends from the cerebral aqueduct to the obex, and is filled with cerebrospinal fluid (CSF).

A cranial nerve nucleus is a collection of neurons in the brain stem that is associated with one or more of the cranial nerves. Axons carrying information to and from the cranial nerves form a synapse first at these nuclei. Lesions occurring at these nuclei can lead to effects resembling those seen by the severing of nerve(s) they are associated with. All the nuclei except that of the trochlear nerve supply nerves of the same side of the body.

Fazio–Londe disease (FLD), also called progressive bulbar palsy of childhood, is a very rare inherited motor neuron disease of children and young adults and is characterized by progressive paralysis of muscles innervated by cranial nerves. FLD, along with Brown–Vialetto–Van Laere syndrome (BVVL), are the two forms of infantile progressive bulbar palsy, a type of progressive bulbar palsy in children.
Progressive bulbar palsy (PBP) is a medical condition. It belongs to a group of disorders known as motor neuron diseases. PBP is a disease that attacks the nerves supplying the bulbar muscles. These disorders are characterized by the degeneration of motor neurons in the cerebral cortex, spinal cord, brain stem, and pyramidal tracts. This specifically involves the glossopharyngeal nerve (IX), vagus nerve (X), and hypoglossal nerve (XII).
Pseudobulbar palsy is a medical condition characterized by the inability to control facial movements and caused by a variety of neurological disorders. Patients experience difficulty chewing and swallowing, have increased reflexes and spasticity in tongue and the bulbar region, and demonstrate slurred speech, sometimes also demonstrating uncontrolled emotional outbursts.

Foix–Chavany–Marie syndrome (FCMS), also known as bilateral opercular syndrome, is a neuropathological disorder characterized by paralysis of the facial, tongue, pharynx, and masticatory muscles of the mouth that aid in chewing. The disorder is primarily caused by thrombotic and embolic strokes, which cause a deficiency of oxygen in the brain. As a result, bilateral lesions may form in the junctions between the frontal lobe and temporal lobe, the parietal lobe and cortical lobe, or the subcortical region of the brain. FCMS may also arise from defects existing at birth that may be inherited or nonhereditary. Symptoms of FCMS can be present in a person of any age and it is diagnosed using automatic-voluntary dissociation assessment, psycholinguistic testing, neuropsychological testing, and brain scanning. Treatment for FCMS depends on the onset, as well as on the severity of symptoms, and it involves a multidisciplinary approach.

The dorsal nucleus of vagus nerve is a cranial nerve nucleus of the vagus nerve situated in the medulla oblongata of the brainstem ventral to the floor of the fourth ventricle. It contains nerve cell bodies of parasympathetic neurons of CN X that provide parasympathetic innervation to the gastrointestinal tract and lungs as well as other thoracic and abdominal organs. These functions include, among others, bronchoconstriction and gland secretion.

In neuroanatomy, the medullary pyramids are paired white matter structures of the brainstem's medulla oblongata that contain motor fibers of the corticospinal and corticobulbar tracts – known together as the pyramidal tracts. The lower limit of the pyramids is marked when the fibers cross (decussate).
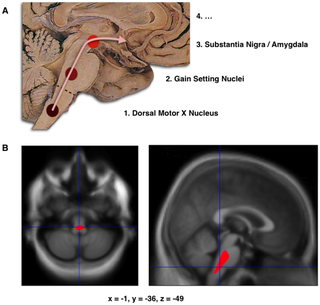
Braak staging refers to two methods used to classify the degree of pathology in Parkinson's disease and Alzheimer's disease. These methods are used both in research and for the clinical diagnosis of these diseases and are obtained by performing an autopsy of the brain.
