Related Research Articles

Tetralogy of Fallot (TOF), formerly known as Steno-Fallot tetralogy, is a congenital heart defect characterized by four specific cardiac defects. Classically, the four defects are:
Hypertrophic cardiomyopathy is a condition in which muscle tissues of the heart become thickened without an obvious cause. The parts of the heart most commonly affected are the interventricular septum and the ventricles. This results in the heart being less able to pump blood effectively and also may cause electrical conduction problems. Specifically, within the bundle branches that conduct impulses through the interventricular septum and into the Purkinje fibers, as these are responsible for the depolarization of contractile cells of both ventricles.
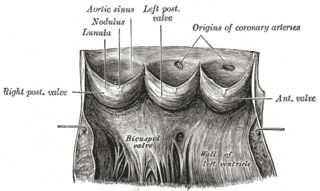
Aneurysm of the aortic sinus, also known as the sinus of Valsalva, is a rare abnormality of the aorta, the largest artery in the body. The aorta normally has three small pouches that sit directly above the aortic valve, and an aneurysm of one of these sinuses is a thin-walled swelling. Aneurysms may affect the right (65–85%), non-coronary (10–30%), or rarely the left coronary sinus. These aneurysms may not cause any symptoms but if large can cause shortness of breath, palpitations or blackouts. Aortic sinus aneurysms can burst or rupture into adjacent cardiac chambers, which can lead to heart failure if untreated.
Mitral regurgitation (MR), also known as mitral insufficiency or mitral incompetence, is a form of valvular heart disease in which the mitral valve is insufficient and does not close properly when the heart pumps out blood. It is the abnormal leaking of blood backwards – regurgitation from the left ventricle, through the mitral valve, into the left atrium, when the left ventricle contracts. Mitral regurgitation is the most common form of valvular heart disease.

A rhabdomyoma is a benign tumor of striated muscle. Rhabdomyomas may be either cardiac or extracardiac. Extracardiac forms of rhabdomyoma are sub-classified into three distinct types: adult type, fetal type, and genital type.

Angiosarcoma is a rare and aggressive cancer that starts in the endothelial cells that line the walls of blood vessels or lymphatic vessels. Since they are made from vascular lining, they can appear anywhere and at any age, but older people are more commonly affected, and the skin is the most affected area, with approximately 60% of cases being cutaneous (skin). Specifically, the scalp makes up ~50% of angiosarcoma cases, but this is still <0.1% of all head and neck tumors. Since angiosarcoma is an umbrella term for many types of tumor that vary greatly in origin and location, many symptoms may occur, from completely asymptomatic to non-specific symptoms like skin lesions, ulceration, shortness of breath and abdominal pain. Multiple-organ involvement at time of diagnosis is common and makes it difficult to ascertain origin and how to treat it.

Atrioventricular septal defect (AVSD) or atrioventricular canal defect (AVCD), also known as "common atrioventricular canal" or "endocardial cushion defect" (ECD), is characterized by a deficiency of the atrioventricular septum of the heart that creates connections between all four of its chambers. It is a very specific combination of 3 defects:

A pericardial effusion is an abnormal accumulation of fluid in the pericardial cavity. The pericardium is a two-part membrane surrounding the heart: the outer fibrous connective membrane and an inner two-layered serous membrane. The two layers of the serous membrane enclose the pericardial cavity between them. This pericardial space contains a small amount of pericardial fluid, normally 15-50 mL in volume. The pericardium, specifically the pericardial fluid provides lubrication, maintains the anatomic position of the heart in the chest, and also serves as a barrier to protect the heart from infection and inflammation in adjacent tissues and organs.

A mediastinal tumor is a tumor in the mediastinum, the cavity that separates the lungs from the rest of the chest. It contains the heart, esophagus, trachea, thymus, and aorta. The most common mediastinal masses are thymoma, usually found in the anterior mediastinum, followed by neurogenic Timor (15–20%) located in the anterior mediastinum. Lung cancer typically spreads to the lymph nodes in the mediastinum.

Nevoid basal-cell carcinoma syndrome (NBCCS) is a rare inherited medical condition involving defects within multiple body systems such as the skin, nervous system, eyes, endocrine system, and bones. People with NBCCS are prone to developing various cancers, including a common and usually non-life-threatening form of non-melanoma skin cancer called basal-cell carcinomas (BCCs). Only about 10% of people with the condition do not develop BCCs; the vast majority of patients develop numerous BCCs.

Primary tumors of the heart are extremely rare tumors that arise from the normal tissues that make up the heart. The incidence of primary cardiac tumors has been found to be approximately 0.02%. This is in contrast to secondary tumors of the heart, which are typically either metastatic from another part of the body, or infiltrate the heart via direct extension from the surrounding tissues. Metastatic tumors to the heart are about 20 times more common than primary cardiac tumors.

A colloid cyst is a non-malignant tumor in the brain. It consists of a gelatinous material contained within a membrane of epithelial tissue. It is almost always found just posterior to the foramen of Monro in the anterior aspect of the third ventricle, originating from the roof of the ventricle. Because of its location, it can cause obstructive hydrocephalus and increased intracranial pressure. Colloid cysts represent 0.5–1.0% of intracranial tumors.
Shone's syndrome is a rare congenital heart defect described by Shone in 1963. In the complete form, four left-sided defects are present:

Thymic carcinoma, or type C thymoma, is a malignancy of the thymus. It is a rare cancer that is often diagnosed at advanced stages. Recurrence following treatment is common, and thymic carcinoma is associated with a poor prognosis.
A papillary fibroelastoma is a primary tumor of the heart that typically involves one of the heart valves. Papillary fibroelastomas, while considered uncommon, make up about 10 percent of all primary tumors of the heart. They are the third most common type of primary tumor of the heart, behind cardiac myxomas and cardiac lipomas.

Anomalous left coronary artery from the pulmonary artery is a rare congenital anomaly occurring in approximately 1 in 300,000 liveborn children. The diagnosis comprises between 0.24 and 0.46% of all cases of congenital heart disease. The anomalous left coronary artery (LCA) usually arises from the pulmonary artery instead of the aortic sinus. In fetal life, the high pressure in the pulmonic artery and the fetal shunts enable oxygen-rich blood to flow in the LCA. By the time of birth, the pressure will decrease in the pulmonic artery and the child will have a postnatal circulation. The myocardium, which is supplied by the LCA, will therefore be dependent on collateral blood flow from the other coronary arteries, mainly the RCA. Because the pressure in RCA exceeds the pressure in LCA a collateral circulation will increase. This situation ultimately can lead to blood flowing from the RCA into the LCA retrograde and into the pulmonary artery, thus forming a left-to-right shunt.

Pleomorphic xanthoastrocytoma (PXA) is a brain tumor that occurs most frequently in children and teenagers. At Boston Children's Hospital, the average age at diagnosis is 12 years.
Ectopic thymus is a condition where thymus tissue is found in an abnormal location. It usually does not cause symptoms, but may leads to a mass in the neck that may compress the trachea and the esophagus. It is thought to be the result of either a failure of descent or a failure of involution of normal thymus tissue. It may be diagnosed with radiology, such as an ultrasound or magnetic resonance imaging. If it causes illness, surgery can be used to remove it. Recurrence after surgery is very unlikely.

The ovarian fibroma, also fibroma, is a benign sex cord-stromal tumour.

A cavernous liver hemangioma or hepatic hemangioma is a benign tumor of the liver composed of large vascular spaces lined by monolayer hepatic endothelial cells. It is the most common benign liver tumour, and is usually asymptomatic and diagnosed incidentally on radiological imaging or during laparotomy for other intra-abdominal issues. Liver hemangiomas are thought to be congenital in origin with an incidence rate of 0.4 – 7.3% as reported in autopsy series.
References
- 1 2 3 4 5 6 Zheng, Xing-Ju; Song, Bin (October 2018). "Left ventricle primary cardiac fibroma in an adult: A case report". Oncology Letters. 16 (4): 5463–5465. doi:10.3892/ol.2018.9260. ISSN 1792-1074. PMC 6144884 . PMID 30250618.
- ↑ Rajput, Furqan A.; Limaiem, Faten (2019), "Cardiac Fibroma", StatPearls, StatPearls Publishing, PMID 30725766 , retrieved 2019-11-05
- 1 2 Reference, Genetics Home. "Gorlin syndrome". Genetics Home Reference. Retrieved 2019-11-05.
- 1 2 3 4 Bruce, C. J. (2011-01-15). "Cardiac tumours: diagnosis and management". Heart. 97 (2): 151–160. doi:10.1136/hrt.2009.186320. ISSN 1355-6037. PMID 21163893. S2CID 43398607.
- 1 2 Cho, John M; Danielson, Gordon K; Puga, Francisco J; Dearani, Joseph A; McGregor, Christopher GA; Tazelaar, Henry D; Hagler, Donald J (December 2003). "Surgical resection of ventricular cardiac fibromas: early and late results". The Annals of Thoracic Surgery. 76 (6): 1929–1934. doi:10.1016/s0003-4975(03)01196-2. ISSN 0003-4975. PMID 14667615.
- 1 2 3 4 5 Torimitsu, Suguru; Nemoto, Tetsuo; Wakayama, Megumi; Okubo, Yoichiro; Yokose, Tomoyuki; Kitahara, Kanako; Ozawa, Tsukasa; Nakayama, Haruo; Shinozaki, Minoru; Sasai, Daisuke; Ishiwatari, Takao (2012). "Literature survey on epidemiology and pathology of cardiac fibroma". European Journal of Medical Research. 17 (1): 5. doi: 10.1186/2047-783x-17-5 . ISSN 2047-783X. PMC 3351722 . PMID 22472419.
- 1 2 Nwachukwu, Harriet; Li, Alice; Nair, Vidhya; Nguyen, Elsie; David, Tirone E.; Butany, Jagdish (July 2011). "Cardiac fibroma in adults". Cardiovascular Pathology. 20 (4): e146–e152. doi:10.1016/j.carpath.2010.08.006. ISSN 1054-8807. PMID 20934889.
- 1 2 Parmley, Loren F.; Salley, Robert K.; Williams, J.Powell; Head, G.Bruce (April 1988). "The clinical spectrum of cardiac fibroma with diagnostic and surgical considerations: Noninvasive imaging enhances management". The Annals of Thoracic Surgery. 45 (4): 455–465. doi: 10.1016/s0003-4975(98)90028-5 . ISSN 0003-4975. PMID 3281617.
- ↑ "Cardiac Fibroma images, diagnosis, treatment options, answer review - Thoracic Imaging". www.vcuthoracicimaging.com. Archived from the original on 2022-07-24. Retrieved 2019-11-05.
- 1 2 Basso, Cristina; Valente, Marialuisa; Thiene, Gaetano (2012-11-28). Cardiac Tumor Pathology. Springer Science & Business Media. ISBN 9781627031431.
- ↑ Heath, D. (1969-09-01). "Cardiac fibroma". Heart. 31 (5): 656–658. doi:10.1136/hrt.31.5.656. ISSN 1355-6037. PMC 487558 . PMID 5351306.
- ↑ "Cardiac Fibroma". DoveMed. Retrieved 2017-11-06.
- 1 2 "Cardiac Tumors | Cleveland Clinic". Cleveland Clinic. Retrieved 2017-12-13.
- 1 2 Borodinova O, Ostras O, Raad T, Yemets I (March 2017). "Successful Surgical Excision of a Large Cardiac Fibroma in an Asymptomatic Child". World J Pediatr Congenit Heart Surg. 8 (2): 235–238. doi:10.1177/2150135116634287. PMID 27143716. S2CID 37344382.
- 1 2 3 Ying L, Lin R, Gao Z, Qi J, Zhang Z, Gu W (April 2016). "Primary cardiac tumors in children: a center's experience". J Cardiothorac Surg. 11 (1): 52. doi: 10.1186/s13019-016-0448-5 . PMC 4827228 . PMID 27067427.