
A nail disease or onychosis is a disease or deformity of the nail. Although the nail is a structure produced by the skin and is a skin appendage, nail diseases have a distinct classification as they have their own signs and symptoms which may relate to other medical conditions. Some nail conditions that show signs of infection or inflammation may require medical assistance.

Onychomycosis, also known as tinea unguium, is a fungal infection of the nail. Symptoms may include white or yellow nail discoloration, thickening of the nail, and separation of the nail from the nail bed. Fingernails may be affected, but it is more common for toenails. Complications may include cellulitis of the lower leg. A number of different types of fungus can cause onychomycosis, including dermatophytes and Fusarium. Risk factors include athlete's foot, other nail diseases, exposure to someone with the condition, peripheral vascular disease, and poor immune function. The diagnosis is generally suspected based on the appearance and confirmed by laboratory testing.
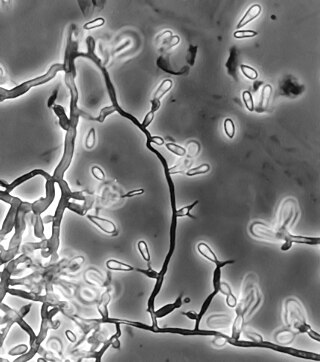
Candida parapsilosis is a fungal species of yeast that has become a significant cause of sepsis and of wound and tissue infections in immunocompromised people. Unlike Candida albicans and Candida tropicalis, C. parapsilosis is not an obligate human pathogen, having been isolated from nonhuman sources such as domestic animals, insects and soil. C. parapsilosis is also a normal human commensal and it is one of the fungi most frequently isolated from human hands. There are several risk factors that can contribute to C. parapsilosis colonization. Immunocompromised individuals and surgical patients, particularly those undergoing surgery of the gastrointestinal tract, are at high risk for infection with C. parapsilosis. There is currently no consensus on the treatment of invasive candidiasis caused by C. parapsilosis, although the therapeutic approach typically includes the removal of foreign bodies such as implanted prostheses and the administration of systemic antifungal therapy. Amphotericin B and Fluconazole are often used in the treatment of C. parapsilosis infection.
A skin infection is an infection of the skin in humans and other animals, that can also affect the associated soft tissues such as loose connective tissue and mucous membranes. They comprise a category of infections termed skin and skin structure infections (SSSIs), or skin and soft tissue infections (SSTIs), and acute bacterial SSSIs (ABSSSIs). They are distinguished from dermatitis, although skin infections can result in skin inflammation.
Fusarium proliferatum is a fungal plant pathogen infecting crops and also can affect humans as well.
Pathogenic fungi are fungi that cause disease in humans or other organisms. Although fungi are eukaryotic, many pathogenic fungi are microorganisms. Approximately 300 fungi are known to be pathogenic to humans; their study is called "medical mycology". Fungal infections are estimated to kill more people than either tuberculosis or malaria—about two million people per year.

Periungual warts are warts that cluster around the fingernail or toenail. They appear as thickened, fissured cauliflower-like skin around the nail plate. Periungual warts often cause loss of the cuticle and paronychia. Nail biting increases susceptibility to these warts.

Majocchi's granuloma is a skin condition characterized by deep, pustular plaques, and is a form of tinea corporis. It is a localized form of fungal folliculitis. Lesions often have a pink and scaly central component with pustules or folliculocentric papules at the periphery. The name comes from Domenico Majocchi, who discovered the disorder in 1883. Majocchi was a professor of dermatology at the University of Parma and later the University of Bologna. This disease is most commonly caused by filamentous fungi in the genus Trichophyton.

The Microascales are an order of fungi in the class Sordariomycetes, subclass Hypocreomycetidae. This is a relatively small order of mostly saprobic fungi that live in soil, rotting vegetation and dung. Some species are plant pathogens, such as Ceratocystis fimbriata, transmitted by beetles to living trees and causing cacao wilt and many other economically important diseases. Species in the genus Pseudallescheria are pathogenic to humans The order was circumscribed in 1980. Wijayawardene et al. in 2020 added more families and genera to the order.
Ochroconis gallopava, also called Dactylaria gallopava or Dactylaria constricta var. gallopava, is a member of genus Dactylaria. Ochroconis gallopava is a thermotolerant, darkly pigmented fungus that causes various infections in fowls, turkeys, poults, and immunocompromised humans first reported in 1986. Since then, the fungus has been increasingly reported as an agent of human disease especially in recipients of solid organ transplants. Ochroconis gallopava infection has a long onset and can involve a variety of body sites. Treatment of infection often involves a combination of antifungal drug therapy and surgical excision.

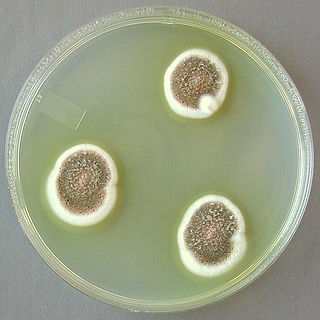
Paecilomyces variotii, also known by the name Byssochlamys spectabilis for the sexual state, is a common environmental mold from the Phylum Ascomycota. It is widespread in the environment and can be found in composts, soils and wood, as well es a common environmental contaminant in indoor air and carpet dust. Ascospores of the sexual state of P. variotii are strongly heat-resistant. As such the fungus is a common contaminant of heat-treated foods and juices. Paecilomyces variotii has been associated with a number of infective diseases of humans and animals.

Onychocola canadensis is a relative of the dermatophyte and an occasionally causes onychomycosis. It was described in 1990 from 3 clinical reports in Canada.
Aspergillus ustus is a microfungus and member of the division Ascomycota. It is commonly found in indoor environments and soil. Isolated cases of human infection resulting from A. ustus have been described; however the majority of these are nail infections.
Scedosporiosis is the general name for any mycosis – i.e., fungal infection – caused by a fungus from the genus Scedosporium. Current population-based studies suggest Scedosporium prolificans and Scedosporium apiospermum to be among the most common infecting agents from the genus, although infections caused by other members thereof are not unheard of. The latter is an asexual form (anamorph) of another fungus, Pseudallescheria boydii. The former is a "black yeast", currently not characterized as well, although both of them have been described as saprophytes.

Neoscytalidium dimidiatum was first described in 1933 as Hendersonula toruloidea from diseased orchard trees in Egypt. Decades later, it was determined to be a causative agent of human dermatomycosis-like infections and foot infections predominantly in tropical areas; however the fungus is considered to be widespread. A newer name, Scytalidium dimidiatum, was applied to a synanamorph of Nattrassia mangiferae, otherwise known as Neofusicoccum mangiferae. Substantial confusion has arisen in the literature on this fungus resulting from the use of multiple different names including Torula dimidiata, Fusicoccum dimidiatum, Scytalidium dimidiatum, and Hendersonula toruloidea. Additionally, Scytalidium lignicola and Scytalidium lignicolum are often considered earlier names of N. dimidiatum.

Epidermophyton floccosum is a filamentous fungus that causes skin and nail infections in humans. This anthropophilic dermatophyte can lead to diseases such as tinea pedis, tinea cruris, tinea corporis and onychomycosis. Diagnostic approaches of the fungal infection include physical examination, culture testing, and molecular detection. Topical antifungal treatment, such as the use of terbinafine, itraconazole, voriconazole, and ketoconazole, is often effective.
Microascus manginii is a filamentous fungal species in the genus Microascus. It produces both sexual (teleomorph) and asexual (anamorph) reproductive stages known as M. manginii and Scopulariopsis candida, respectively. Several synonyms appear in the literature because of taxonomic revisions and re-isolation of the species by different researchers. M. manginii is saprotrophic and commonly inhabits soil, indoor environments and decaying plant material. It is distinguishable from closely related species by its light colored and heart-shaped ascospores used for sexual reproduction. Scopulariopsis candida has been identified as the cause of some invasive infections, often in immunocompromised hosts, but is not considered a common human pathogen. There is concern about amphotericin B resistance in S. candida.
Arthrographis kalrae is an ascomycetous fungus responsible for human nail infections described in 1938 by Cochet as A. langeronii. A. kalrae is considered a weak pathogen of animals including human restricted to the outermost keratinized layers of tissue. Infections caused by this species are normally responsive to commonly used antifungal drugs with only very rare exceptions.
Emmonsiosis, also known as emergomycosis, is a systemic fungal infection that can affect the lungs, generally always affects the skin and can become widespread. The lesions in the skin look like small red bumps and patches with a dip, ulcer and dead tissue in the centre.
