Endometrial cancer is a cancer that arises from the endometrium. It is the result of the abnormal growth of cells that have the ability to invade or spread to other parts of the body. The first sign is most often vaginal bleeding not associated with a menstrual period. Other symptoms include pain with urination, pain during sexual intercourse, or pelvic pain. Endometrial cancer occurs most commonly after menopause.

Ovarian cancer is a cancerous tumor of an ovary. It may originate from the ovary itself or more commonly from communicating nearby structures such as fallopian tubes or the inner lining of the abdomen. The ovary is made up of three different cell types including epithelial cells, germ cells, and stromal cells. When these cells become abnormal, they have the ability to divide and form tumors. These cells can also invade or spread to other parts of the body. When this process begins, there may be no or only vague symptoms. Symptoms become more noticeable as the cancer progresses. These symptoms may include bloating, vaginal bleeding, pelvic pain, abdominal swelling, constipation, and loss of appetite, among others. Common areas to which the cancer may spread include the lining of the abdomen, lymph nodes, lungs, and liver.
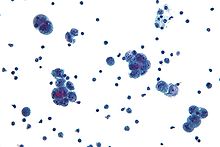
A psammoma body is a round collection of calcium, seen microscopically. The term is derived from the Greek word ψάμμος (psámmos), meaning "sand".

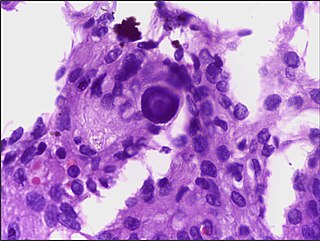
Ovarian clear-cell carcinoma, or clear-cell carcinoma of the ovary, also called ovarian clear-cell adenocarcinoma, is one of several subtypes of ovarian carcinoma – a subtype of epithelial ovarian cancer, in contrast to non-epithelial cancers. According to research, most ovarian cancers start at the epithelial layer which is the lining of the ovary. Within this epithelial group ovarian clear-cell carcinoma makes up 5–10%.

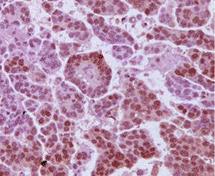
A serous tumour is a neoplasm that typically has papillary to solid formations of tumor cells with crowded nuclei, and which typically arises on the modified Müllerian-derived serous membranes that surround the ovaries in females. Such ovarian tumors are part of the surface epithelial-stromal tumour group of ovarian tumors. They are common neoplasms with a strong tendency to occur bilaterally, and they account for approximately a quarter of all ovarian tumors.

Surface epithelial-stromal tumors are a class of ovarian neoplasms that may be benign or malignant. Neoplasms in this group are thought to be derived from the ovarian surface epithelium or from ectopic endometrial or fallopian tube (tubal) tissue. Tumors of this type are also called ovarian adenocarcinoma. This group of tumors accounts for 90% to 95% of all cases of ovarian cancer; however is mainly only found in postmenopausal women with the exception of the United States where 7% of cases occur in women under the age of 40. Serum CA-125 is often elevated but is only 50% accurate so it is not a useful tumor marker to assess the progress of treatment. 75% of women with epithelial ovarian cancer are found within the advanced-stages; however younger patients are more likely to have better prognoses than older patients.

Vulvar cancer is a cancer of the vulva, the outer portion of the female genitals. It most commonly affects the labia majora. Less often, the labia minora, clitoris, or Bartholin's glands are affected. Symptoms include a lump, itchiness, changes in the skin, or bleeding from the vulva.
Gynecologic oncology is a specialized field of medicine that focuses on cancers of the female reproductive system, including ovarian cancer, uterine cancer, vaginal cancer, cervical cancer, and vulvar cancer. As specialists, they have extensive training in the diagnosis and treatment of these cancers.
Gynecologic cancer is a type of cancer that affects the female reproductive system, including ovarian cancer, uterine cancer, vaginal cancer, cervical cancer, and vulvar cancer.
Steven A. Vasilev is an American gynecologist, specializing in gynecologic oncology. He has served as Professor and Director of Integrative Medicine and Gynecologic Oncology at John Wayne Cancer Institute-Providence Saint John’s Health Center, Professor at John Wayne Cancer Institute in Santa Monica, California, and Professor at Loma Linda University School of Medicine faculty. Vasilev is a proponent of minimally invasive (laparoscopic) and robotic cancer surgery and complex pelvic surgery and has published research on medical and surgical therapies, integrative medicine, and screening for cervical cancer and human papilloma virus (HPV)

Primary fallopian tube cancer (PFTC), also known as tubal cancer, is a malignant neoplasm that originates from the fallopian tube. Along with primary ovarian and peritoneal carcinomas, it is grouped under epithelial ovarian cancers, cancers of the ovary that originate from a fallopian tube precursor.

Uterine serous carcinoma is a malignant form of serous tumor that originates in the uterus. It is an uncommon form of endometrial cancer that typically arises in postmenopausal women. It is typically diagnosed on endometrial biopsy, prompted by post-menopausal bleeding.
Uterine clear-cell carcinoma (CC) is a rare form of endometrial cancer with distinct morphological features on pathology; it is aggressive and has high recurrence rate. Like uterine papillary serous carcinoma CC does not develop from endometrial hyperplasia and is not hormone sensitive, rather it arises from an atrophic endometrium. Such lesions belong to the type II endometrial cancers.
A borderline tumor, sometimes called low malignant potential (LMP) tumor, is a distinct but yet heterogeneous group of tumors defined by their histopathology as atypical epithelial proliferation without stromal invasion. It generally refers to such tumors in the ovary but borderline tumors may rarely occur at other locations as well.

Adenosarcoma is a rare malignant tumor that occurs in women of all age groups, but most commonly post-menopause. Adenosarcoma arises from mesenchymal tissue and has a mixture of the tumoral components of an adenoma, a tumor of epithelial origin, and a sarcoma, a tumor originating from connective tissue. The adenoma, or epithelial component of the tumor, is benign, while the sarcomatous stroma is malignant. The most common site of adenosarcoma formation is the uterus, but it can also occur in the cervix and ovaries. It more rarely arises in the vagina and fallopian tubes as well as primary pelvic or peritoneal sites, such as the omentum, especially in those with a history of endometriosis. The rare cases of adenosarcoma outside the female genital tract usually occur in the liver, bladder, kidney, as well as the intestine and are typically associated with endometriosis.
High-grade serous carcinoma (HGSC) is a type of tumour that arises from the serous epithelial layer in the abdominopelvic cavity and is mainly found in the ovary. HGSCs make up the majority of ovarian cancer cases and have the lowest survival rates. HGSC is distinct from low-grade serous carcinoma (LGSC) which arises from ovarian tissue, is less aggressive and is present in stage I ovarian cancer where tumours are localised to the ovary.

Gynecologic cancer disparities in the United States refer to differences in incidence, prevalence, and mortality from gynecologic cancers between population groups. The five main types of gynecologic cancer include cervical cancer, ovarian cancer, endometrial cancer, vaginal cancer, and vulvar cancer. For patients with these and other gynecologic malignancies within the United States, disparities across the care continuum by socioeconomic status and racial/ethnic background have been previously identified and studied. The causes behind these disparities are multifaceted and a complex interplay of systemic differences in health as well as individual patient factors such as cultural, educational, and economic barriers.
Bradley J. Monk is an American gynecologic oncologist, academician and researcher. He is a Professor on the Clinical Scholar Track in the Department of Obstetrics and Gynecology at the University of Arizona College of Medicine in Phoenix, Arizona, as well as at the Creighton University School of Medicine in Omaha, Nebraska. He also serves as Director of the Division of Gynecologic Oncology at the St. Joseph's Hospital and Medical Center in Phoenix.

The SEE-FIM protocol is a pathology dissection protocol for Sectioning and Extensively Examining the Fimbria (SEE-FIM). This protocol is intended to provide for the optimal microscopic examination of the distal fallopian tube (fimbria) to identify either cancerous or precancerous conditions in this organ.

Ovarian squamous cell carcinoma (oSCC) or squamous ovarian carcinoma (SOC) is a rare tumor that accounts for 1% of ovarian cancers. Included in the World Health Organization's classification of ovarian cancer, it mainly affects women above 45 years of age. Survival depends on how advanced the disease is and how different or similar the individual cancer cells are.