Probiotics are live microorganisms promoted with claims that they provide health benefits when consumed, generally by improving or restoring the gut microbiota. Probiotics are considered generally safe to consume, but may cause bacteria-host interactions and unwanted side effects in rare cases. There is some evidence that probiotics are beneficial for some conditions, but there is little evidence for many of the health benefits claimed for them.

Colitis is swelling or inflammation of the large intestine (colon). Colitis may be acute and self-limited or long-term. It broadly fits into the category of digestive diseases.

The Clostridia are a highly polyphyletic class of Bacillota, including Clostridium and other similar genera. They are distinguished from the Bacilli by lacking aerobic respiration. They are obligate anaerobes and oxygen is toxic to them. Species of the class Clostridia are often but not always Gram-positive and have the ability to form spores. Studies show they are not a monophyletic group, and their relationships are not entirely certain. Currently, most are placed in a single order called Clostridiales, but this is not a natural group and is likely to be redefined in the future.

Fecal microbiota transplant (FMT), also known as a stool transplant, is the process of transferring fecal bacteria and other microbes from a healthy individual into another individual. FMT is an effective treatment for Clostridioides difficile infection (CDI). For recurrent CDI, FMT is more effective than vancomycin alone, and may improve the outcome after the first index infection.

Rifaximin, is a non-absorbable, broad spectrum antibiotic mainly used to treat travelers' diarrhea. It is based on the rifamycin antibiotics family. Since its approval in Italy in 1987, it has been licensed in over more than 30 countries for the treatment of a variety of gastrointestinal diseases like irritable bowel syndrome, and hepatic encephalopathy. It acts by inhibiting RNA synthesis in susceptible bacteria by binding to the RNA polymerase enzyme. This binding blocks translocation, which stops transcription. It is marketed under the brand name Xifaxan by Salix Pharmaceuticals.
Antibiotic-associated diarrhea (AAD) results from an imbalance in the colonic microbiota caused by antibiotics. Microbiotal alteration changes carbohydrate metabolism with decreased short-chain fatty acid absorption and an osmotic diarrhea as a result. Another consequence of antibiotic therapy leading to diarrhea is overgrowth of potentially pathogenic organisms such as Clostridium difficile. It is defined as frequent loose and watery stools with no other complications.
Dysbiosis is characterized by a disruption to the microbiome resulting in an imbalance in the microbiota, changes in their functional composition and metabolic activities, or a shift in their local distribution. For example, a part of the human microbiota such as the skin flora, gut flora, or vaginal flora, can become deranged, with normally dominating species underrepresented and normally outcompeted or contained species increasing to fill the void. Similar to the human gut microbiome, diverse microbes colonize the plant rhizosphere, and dysbiosis in the rhizosphere, can negatively impact plant health. Dysbiosis is most commonly reported as a condition in the gastrointestinal tract or plant rhizosphere.
Saccharomyces boulardii is a tropical yeast first isolated from lychee and mangosteen fruit peel in 1923 by French scientist Henri Boulard. Although early reports claimed distinct taxonomic, metabolic, and genetic properties, S. boulardii is genetically a grouping of S. cerevisiae strains, sharing >99% genomic relatedness, giving the synonym S. cerevisiae var. boulardii.
Clostridioides difficile toxin B (TcdB) is a cytotoxin produced by the bacteria Clostridioides difficile. It is one of two major kinds of toxins produced by C. difficile, the other being a related enterotoxin. Both are very potent and lethal.

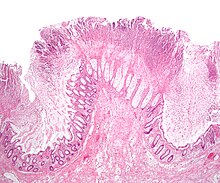
Clostridioides difficile toxin A (TcdA) is a toxin produced by the bacteria Clostridioides difficile, formerly known as Clostridium difficile. It is similar to Clostridium difficile Toxin B. The toxins are the main virulence factors produced by the gram positive, anaerobic, Clostridioides difficile bacteria. The toxins function by damaging the intestinal mucosa and cause the symptoms of C. difficile infection, including pseudomembranous colitis.

Fidaxomicin, sold under the brand name Dificid among others, is the first member of a class of narrow spectrum macrocyclic antibiotic drugs called tiacumicins. It is a fermentation product obtained from the actinomycete Dactylosporangium aurantiacum subspecies hamdenesis. Fidaxomicin is minimally absorbed into the bloodstream when taken orally, is bactericidal, and selectively eradicates pathogenic Clostridioides difficile with relatively little disruption to the multiple species of bacteria that make up the normal, healthy intestinal microbiota. The maintenance of normal physiological conditions in the colon may reduce the probability of recurrence of Clostridioides difficile infection.
Colitis X, equine colitis X or peracute toxemic colitis is a catchall term for various fatal forms of acute or peracute colitis found in horses, but particularly a fulminant colitis where clinical signs include sudden onset of severe diarrhea, abdominal pain, shock, and dehydration. Death is common, with 90–100% mortality, usually in less than 24 hours. The causative factor may be Clostridium difficile, but it also may be caused by other intestinal pathogens. Horses under stress appear to be more susceptible to developing colitis X, and like the condition pseudomembranous colitis in humans, an association with prior antibiotic use also exists. Immediate and aggressive treatment can sometimes save the horse, but even in such cases, 75% mortality is considered a best-case scenario.
Clostridium innocuum is an anaerobic, non-motile, gram-positive bacterium that reproduces by sporulation. While there are over 130 species of Clostridium, C. innocuum is the third most commonly isolated. Although it is not normally considered an aggressive human pathogen, it has been isolated in some disease processes. C. innocuum and other Clostridium line the oropharynx and gastrointestinal tract, and are considered normal gut flora.

Cadazolid is an experimental antibiotic of the oxazolidinone class made by Actelion Pharmaceuticals Ltd. which is effective against Clostridium difficile, a major cause of drug resistant diarrhea in the elderly. Current drug treatments for this infection involve orally delivered antibiotics, principally fidaxomicin, metronidazole and vancomycin; the last two drugs are the principal therapeutic agents in use, but fail in approximately 20 to 45% of the cases. The drug works by inhibiting synthesis of proteins in the bacteria, thus inhibiting the production of toxins and the formation of spores. Cadazolid progressed through to Phase III clinical trials, but in its financial results for Q1 2018, Idorsia mentions that Actelion informed them that "following completion of Phase 3 data analysis of cadazolid - it has decided to discontinue the development of the compound."
Bacteriotherapy is the purposeful use of bacteria or their products in treating an illness. Forms of bacteriotherapy include the use of probiotics, microorganisms that provide health benefits when consumed; fecal matter transplants (FMT) /intestinal microbiota transplant (IMT), the transfer of gut microorganisms from the fecal matter of healthy donors to recipient patients to restore microbiota; or synbiotics which combine prebiotics, indigestible ingredients that promote growth of beneficial microorganisms, and probiotics. Through these methods, the gut microbiota, the community of 300-500 microorganism species that live in the digestive tract of animals aiding in digestion, energy storage, immune function and protection against pathogens, can be recolonized with favorable bacteria, which in turn has therapeutic effects.

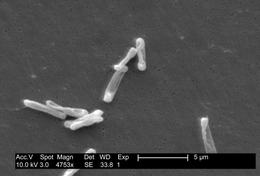
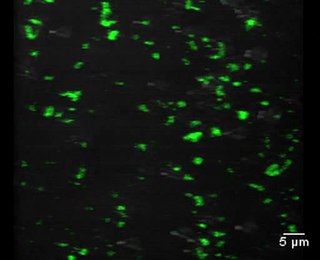
Clostridioides difficile is a bacterium known for causing serious diarrheal infections, and may also cause colon cancer. It is known also as C. difficile, or C. diff, and is a Gram-positive species of spore-forming bacteria. Clostridioides spp. are anaerobic, motile bacteria, ubiquitous in nature and especially prevalent in soil. Its vegetative cells are rod-shaped, pleomorphic, and occur in pairs or short chains. Under the microscope, they appear as long, irregular cells with a bulge at their terminal ends. Under Gram staining, C. difficile cells are Gram-positive and show optimum growth on blood agar at human body temperatures in the absence of oxygen. C. difficile is catalase- and superoxide dismutase-negative, and produces up to three types of toxins: enterotoxin A, cytotoxin B and Clostridioides difficile transferase. Under stress conditions, the bacteria produce spores that are able to tolerate extreme conditions that the active bacteria cannot tolerate.

Ridinilazole is an investigational small molecule antibiotic being evaluated for oral administration to treat Clostridioides difficile infection (CDI). In vitro, it is bactericidal against C. difficile and suppresses bacterial toxin production; the mechanism of action is thought to involve inhibition of cell division. It has properties which are desirable for the treatment of CDI, namely that it is a narrow-spectrum antibiotic which exhibits activity against C. difficile while having little impact on other normal intestinal flora and that it is only minimally absorbed systemically after oral administration. At the time ridinilazole was developed, there were only three antibiotics in use for treating CDI: vancomycin, fidaxomicin, and metronidazole. The recurrence rate of CDI is high, which has spurred research into other treatment options with the aim to reduce the rate of recurrence.
Fecal microbiota, sold under the brand name, Rebyota is used for the prevention of recurrence of Clostridioides difficile infection.
Live fecal microbiota spores, sold under the brand name Vowst, is a fecal microbiota product used to prevent the recurrence of Clostridioides difficile infection.