Non-steroidal anti-inflammatory drugs (NSAID) are members of a therapeutic drug class which reduces pain, decreases inflammation, decreases fever, and prevents blood clots. Side effects depend on the specific drug, its dose and duration of use, but largely include an increased risk of gastrointestinal ulcers and bleeds, heart attack, and kidney disease.
An antipyretic is a substance that reduces fever. Antipyretics cause the hypothalamus to override a prostaglandin-induced increase in temperature. The body then works to lower the temperature, which results in a reduction in fever.

Ibuprofen is a nonsteroidal anti-inflammatory drug (NSAID) that is used to relieve pain, fever, and inflammation. This includes painful menstrual periods, migraines, and rheumatoid arthritis. It may also be used to close a patent ductus arteriosus in a premature baby. It can be used orally or intravenously. It typically begins working within an hour.
Phenacetin is a pain-relieving and fever-reducing drug, which was widely used following its introduction in 1887. It was withdrawn from medicinal use as dangerous from the 1970s.

Kidney disease, or renal disease, technically referred to as nephropathy, is damage to or disease of a kidney. Nephritis is an inflammatory kidney disease and has several types according to the location of the inflammation. Inflammation can be diagnosed by blood tests. Nephrosis is non-inflammatory kidney disease. Nephritis and nephrosis can give rise to nephritic syndrome and nephrotic syndrome respectively. Kidney disease usually causes a loss of kidney function to some degree and can result in kidney failure, the complete loss of kidney function. Kidney failure is known as the end-stage of kidney disease, where dialysis or a kidney transplant is the only treatment option.
Acute kidney injury (AKI), previously called acute renal failure (ARF), is a sudden decrease in kidney function that develops within 7 days, as shown by an increase in serum creatinine or a decrease in urine output, or both.

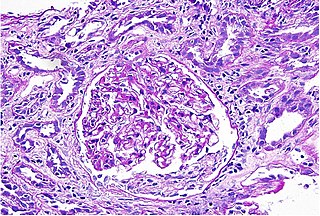
IgA nephropathy (IgAN), also known as Berger's disease, or synpharyngitic glomerulonephritis, is a disease of the kidney and the immune system; specifically it is a form of glomerulonephritis or an inflammation of the glomeruli of the kidney. Aggressive Berger's disease can attack other major organs, such as the liver, skin and heart.
Anti-inflammatory or antiphlogistic is the property of a substance or treatment that reduces inflammation or swelling. Anti-inflammatory drugs, also called anti-inflammatories, make up about half of analgesics. These drugs remedy pain by reducing inflammation as opposed to opioids, which affect the central nervous system to block pain signaling to the brain.

Indometacin, also known as indomethacin, is a nonsteroidal anti-inflammatory drug (NSAID) commonly used as a prescription medication to reduce fever, pain, stiffness, and swelling from inflammation. It works by inhibiting the production of prostaglandins, endogenous signaling molecules known to cause these symptoms. It does this by inhibiting cyclooxygenase, an enzyme that catalyzes the production of prostaglandins.
Nephrotoxicity is toxicity in the kidneys. It is a poisonous effect of some substances, both toxic chemicals and medications, on kidney function. There are various forms, and some drugs may affect kidney function in more than one way. Nephrotoxins are substances displaying nephrotoxicity.
COX-3 is an enzyme that is encoded by the PTGS1 (COX1) gene, but is not functional in humans. COX-3 is the third and most recently discovered cyclooxygenase (COX3050) isozyme, while the first two to be discovered were COX-1 and COX-2. The COX-3 isozyme is encoded by the same gene as COX-1, with the difference that COX-3 retains an intron that is not retained in COX-1.
Thin basement membrane disease is, along with IgA nephropathy, the most common cause of hematuria without other symptoms. The only abnormal finding in this disease is a thinning of the basement membrane of the glomeruli in the kidneys. Its importance lies in the fact that it has a benign prognosis, with patients maintaining a normal kidney function throughout their lives.
Interstitial nephritis, also known as tubulointerstitial nephritis, is inflammation of the area of the kidney known as the renal interstitium, which consists of a collection of cells, extracellular matrix, and fluid surrounding the renal tubules. It is also known as intestinal nephritis because the clinical picture may include mesenteric lymphadenitis in some cases of acute pyelonephritis. More specifically, in case of recurrent urinary tract infection, secondary infection can spread to adjacent intestine. In addition to providing a scaffolding support for the tubular architecture, the interstitium has been shown to participate in the fluid and electrolyte exchange as well as endocrine functions of the kidney.
Phosphate nephropathy or nephrocalcinosis is an adverse renal condition that arises with a formation of phosphate crystals within the kidney's tubules. This renal insufficiency is associated with the use of oral sodium phosphate (OSP) such as C.B. Fleet's Phospho soda and Salix's Visocol, for bowel cleansing prior to a colonoscopy.

Balkan endemic nephropathy (BEN) is a form of interstitial nephritis causing kidney failure. It was first identified in the 1920s among several small, discrete communities along the Danube River and its major tributaries, in the modern countries of Croatia, Bosnia and Herzegovina, Serbia, Kosovo, Romania, and Bulgaria. It is caused by small long-term doses of aristolochic acid in the diet. The disease primarily affects people 30 to 60 years of age. Doses of the toxin are usually low and people moving to endemic areas typically develop the condition only when they have lived there for 10–20 years. People taking higher doses of aristolochic acid have developed kidney failure after shorter durations of exposure.

Renal papillary necrosis is a form of nephropathy involving the necrosis of the renal papilla. Lesions that characterize renal papillary necrosis come from an impairment of the blood supply and from subsequent ischemic necrosis that is diffuse.
A prostaglandin antagonist is a hormone antagonist acting upon one or more prostaglandins, a subclass of eicosanoid compounds which function as signaling molecules in numerous types of animal tissues.
Sickle cell nephropathy is a type of nephropathy associated with sickle cell disease which causes kidney complications as a result of sickling of red blood cells in the small blood vessels. The hypertonic and relatively hypoxic environment of the renal medulla, coupled with the slow blood flow in the vasa recta, favors sickling of red blood cells, with resultant local infarction. Functional tubule defects in patients with sickle cell disease are likely the result of partial ischemic injury to the renal tubules.
Aspirin/paracetamol/caffeine is a combination drug for the treatment of pain, especially tension headache and migraine. It contains aspirin, a non-steroidal anti-inflammatory drug; paracetamol (acetaminophen), an analgesic; and caffeine, a stimulant.
Prostaglandin inhibitors are drugs that inhibit the synthesis of prostaglandin in human body. There are various types of prostaglandins responsible for different physiological reactions such as maintaining the blood flow in stomach and kidney, regulating the contraction of involuntary muscles and blood vessels, and act as a mediator of inflammation and pain. Cyclooxygenase (COX) and Phospholipase A2 are the major enzymes involved in prostaglandin production, and they are the drug targets for prostaglandin inhibitors. There are mainly 2 classes of prostaglandin inhibitors, namely non- steroidal anti- inflammatory drugs (NSAIDs) and glucocorticoids. In the following sections, the medical uses, side effects, contraindications, toxicity and the pharmacology of these prostaglandin inhibitors will be discussed.
