Related Research Articles
A ligament is the fibrous connective tissue that connects bones to other bones. It also connects flight feathers to bones, in dinosaurs and birds. All 30,000 species of amniotes have ligaments.
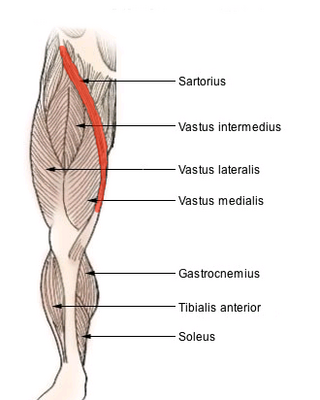
The sartorius muscle is the longest muscle in the human body. It is a long, thin, superficial muscle that runs down the length of the thigh in the anterior compartment.

A fascial compartment is a section within the body that contains muscles and nerves and is surrounded by deep fascia. In the human body, the limbs can each be divided into two segments – the upper limb can be divided into the arm and the forearm and the sectional compartments of both of these – the fascial compartments of the arm and the fascial compartments of the forearm contain an anterior and a posterior compartment. Likewise, the lower limbs can be divided into two segments – the leg and the thigh – and these contain the fascial compartments of the leg and the fascial compartments of the thigh.

A fascia is a generic term for macroscopic membranous bodily structures. Fasciae are classified as superficial, visceral or deep, and further designated according to their anatomical location.

The anterior cruciate ligament (ACL) is one of a pair of cruciate ligaments in the human knee. The two ligaments are called "cruciform" ligaments, as they are arranged in a crossed formation. In the quadruped stifle joint, based on its anatomical position, it is also referred to as the cranial cruciate ligament. The term cruciate is Latin for cross. This name is fitting because the ACL crosses the posterior cruciate ligament to form an "X". It is composed of strong, fibrous material and assists in controlling excessive motion by limiting mobility of the joint. The anterior cruciate ligament is one of the four main ligaments of the knee, providing 85% of the restraining force to anterior tibial displacement at 30 and 90° of knee flexion. The ACL is the most frequently injured ligament in the knee.

The omohyoid muscle is a muscle in the neck. It is one of the infrahyoid muscles. It consists of two bellies separated by an intermediate tendon. Its inferior belly is attached to the scapula; its superior belly is attached to the hyoid bone. Its intermediate tendon is anchored to the clavicle and first rib by a fascial sling. The omohyoid is innervated by the ansa cervicalis of the cervical plexus. It acts to depress the hyoid bone.

An aponeurosis is a flattened tendon by which muscle attaches to bone or fascia. Aponeuroses exhibit an ordered arrangement of collagen fibres, thus attaining high tensile strength in a particular direction while being vulnerable to tensional or shear forces in other directions. They have a shiny, whitish-silvery color, are histologically similar to tendons, and are very sparingly supplied with blood vessels and nerves. When dissected, aponeuroses are papery and peel off by sections. The primary regions with thick aponeuroses are in the ventral abdominal region, the dorsal lumbar region, the ventriculus in birds, and the palmar (palms) and plantar (soles) regions.

The endomysium, meaning within the muscle, is a wispy layer of areolar connective tissue that ensheaths each individual muscle fiber, or muscle cell. It also contains capillaries and nerves. It overlies the muscle fiber's cell membrane: the sarcolemma. Endomysium is the deepest and smallest component of muscle connective tissue. This thin layer helps provide an appropriate chemical environment for the exchange of calcium, sodium, and potassium, which is essential for the excitation and subsequent contraction of a muscle fiber.

The semitendinosus is a long superficial muscle in the back of the thigh. It is so named because it has a very long tendon of insertion. It lies posteromedially in the thigh, superficial to the semimembranosus.

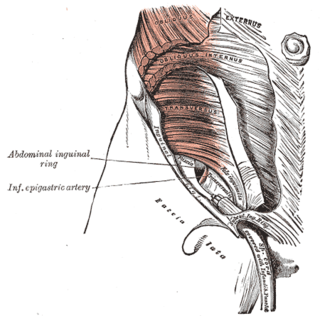
The iliopsoas muscle refers to the joined psoas major and the iliacus muscles. The two muscles are separate in the abdomen, but usually merge in the thigh. They are usually given the common name iliopsoas. The iliopsoas muscle joins to the femur at the lesser trochanter. It acts as the strongest flexor of the hip.

The thoracolumbar fascia is a complex, multilayer arrangement of fascial and aponeurotic layers forming a separation between the paraspinal muscles on one side, and the muscles of the posterior abdominal wall on the other. It spans the length of the back, extending between the neck superiorly and the sacrum inferiorly. It entails the fasciae and aponeuroses of the latissimus dorsi muscle, serratus posterior inferior muscle, abdominal internal oblique muscle, and transverse abdominal muscle.
The fascia lata is the deep fascia of the thigh. It encloses the thigh muscles and forms the outer limit of the fascial compartments of thigh, which are internally separated by the medial intermuscular septum and the lateral intermuscular septum. The fascia lata is thickened at its lateral side where it forms the iliotibial tract, a structure that runs to the tibia and serves as a site of muscle attachment.
The transversalis fascia is the fascial lining of the anterolateral abdominal wall situated between the inner surface of the transverse abdominal muscle, and the preperitoneal fascia. It is directly continuous with the iliac fascia, the internal spermatic fascia, and pelvic fascia.

The fascial compartments of arm refers to the specific anatomical term of the compartments within the upper segment of the upper limb of the body. The upper limb is divided into two segments, the arm and the forearm. Each of these segments is further divided into two compartments which are formed by deep fascia – tough connective tissue septa (walls). Each compartment encloses specific muscles and nerves.

In human male anatomy, the radix or root of the penis is the internal and most proximal portion of the human penis that lies in the perineum. Unlike the pendulous body of the penis, which is suspended from the pubic symphysis, the root is attached to the pubic arch of the pelvis and is not visible externally. It is triradiate in form, consisting of three masses of erectile tissue; the two diverging crura, one on either side, and the median bulb of the penis or urethral bulb. Approximately one third to one half of the penis is embedded in the pelvis and can be felt through the scrotum and in the perineum.
Fascia training describes sports activities and movement exercises that attempt to improve the functional properties of the muscular connective tissues in the human body, such as tendons, ligaments, joint capsules and muscular envelopes. Also called fascia, these tissues take part in a body-wide tensional force transmission network and are responsive to training stimulation. As of 2018 the body-wide continuity of this tensional system has been expressed in an educational manner within the Fascial Net Plastination Project. The FNPP brought together experts in anatomy, dissection, and plastination, and it was the first project of its kind to plastinate a complete human fascia specimen.

The vaginal support structures are those muscles, bones, ligaments, tendons, membranes and fascia, of the pelvic floor that maintain the position of the vagina within the pelvic cavity and allow the normal functioning of the vagina and other reproductive structures in the female. Defects or injuries to these support structures in the pelvic floor leads to pelvic organ prolapse. Anatomical and congenital variations of vaginal support structures can predispose a woman to further dysfunction and prolapse later in life. The urethra is part of the anterior wall of the vagina and damage to the support structures there can lead to incontinence and urinary retention.
Fascial Manipulation is a manual therapy technique developed by Italian physiotherapist Luigi Stecco in the 1980s, aimed at evaluating and treating global fascial dysfunction by restoring normal motion/gliding to the system.
![<span class="mw-page-title-main">Robert Schleip</span> German [[Fascia]] Researcher](https://upload.wikimedia.org/wikipedia/commons/6/6a/RobertSchleip.jpg)
Robert Schleip is a German psychologist, human biologist and author, best known for his research in the field of fascia. His work includes numerous scientific papers and books, which have contributed to the understanding of fascia and its role in musculoskeletal health. He serves as the Director of the Fascia Research Group at both the University of Ulm and the Technical University of Munich. Schleip is also the founding director of the Fascia Research Society, the Research Director of the European Rolfing Association and Vice President of the Ida P. Rolf Research Foundation.

The Fascial Net Plastination Project is an anatomical research initiative established in 2018 aimed at plastinating and studying the human fascial network. The collaboration was initiated by Robert Schleip as a joint effort between Body Worlds, Fascia Research Group, and the Fascia Research Society. The project focuses on preserving the fascia, a complex connective tissue network that plays a crucial role in the human body's structure and function.
References
- ↑ Hedley, Gil (2005). The Integral Anatomy Series Vol. 2: Deep Fascia and Muscle (DVD). Integral Anatomy Productions. Retrieved 2006-07-17.
- ↑ Rolf, Ida P. (1989). Rolfing . Rochester, VT: Healing Arts Press. p. 38. ISBN 0892813350.
- 1 2 Schleip, Robert (2003). "Fascial plasticity – a new neurobiological explanation: Part 1". Journal of Bodywork and Movement Therapies. 7 (1): 11–9. doi:10.1016/S1360-8592(02)00067-0.
- ↑ Gatt, Adrianna; Agarwal, Sanjay; Zito, Patrick M. (2021). "Anatomy, Fascia Layers". StatPearls. StatPearls Publishing.
- ↑ Myers, Thomas W. (2002). Anatomy Trains. London, UK: Churchill Livingstone. p. 15. ISBN 0443063516.
- ↑ Tomasek, James J.; Gabbiani, Giulio; Hinz, Boris; Chaponnier, Christine; Brown, Robert A. (2002). "Myofibroblasts and mechano-regulation of connective tissue remodelling". Nature Reviews Molecular Cell Biology. 3 (5): 349–63. doi:10.1038/nrm809. PMID 11988769.
- ↑ Chaitow, Leon (1988). Soft Tissue Manipulation. Rochester, VT: Healing Arts Press. pp. 26–7. ISBN 0892812761.
- ↑ Schleip, Robert (2003). "Fascial plasticity – a new neurobiological explanation Part 2". Journal of Bodywork and Movement Therapies. 7 (2): 104–16. doi:10.1016/S1360-8592(02)00076-1.
- ↑ Paoletti, Serge (2006). The Fasciae: Anatomy, Dysfunction & Treatment. Seattle, WA: Eastland Press. pp. 138, 147–9. ISBN 093961653X.
- ↑ Wojtys, E. M.; Huston, L. J.; Lindenfeld, T. N.; Hewett, T. E.; Greenfield, M. L. (1998). "Association between the menstrual cycle and anterior cruciate ligament injuries in female athletes". The American Journal of Sports Medicine. 26 (5): 614–9. doi:10.1177/03635465980260050301. PMID 9784805.
- ↑ Heitz, N. A.; Eisenman, P. A.; Beck, C. L.; Walker, J. A. (1999). "Hormonal changes throughout the menstrual cycle and increased anterior cruciate ligament laxity in females". Journal of Athletic Training. 34 (2): 144–9. PMC 1322903 . PMID 16558557.
- ↑ "FR:EIA - Fascial Net Plastination Project". Body Worlds. Retrieved 2024-08-26.