
The small intestine or small bowel is an organ in the gastrointestinal tract where most of the absorption of nutrients from food takes place. It lies between the stomach and large intestine, and receives bile and pancreatic juice through the pancreatic duct to aid in digestion. The small intestine is about 5.5 metres long and folds many times to fit in the abdomen. Although it is longer than the large intestine, it is called the small intestine because it is narrower in diameter.
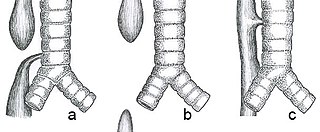
Esophageal atresia is a congenital medical condition that affects the alimentary tract. It causes the esophagus to end in a blind-ended pouch rather than connecting normally to the stomach. It comprises a variety of congenital anatomic defects that are caused by an abnormal embryological development of the esophagus. It is characterized anatomically by a congenital obstruction of the esophagus with interruption of the continuity of the esophageal wall.

Bowel obstruction, also known as intestinal obstruction, is a mechanical or functional obstruction of the intestines which prevents the normal movement of the products of digestion. Either the small bowel or large bowel may be affected. Signs and symptoms include abdominal pain, vomiting, bloating and not passing gas. Mechanical obstruction is the cause of about 5 to 15% of cases of severe abdominal pain of sudden onset requiring admission to hospital.

An upper gastrointestinal series, also called a barium swallow, barium study, or barium meal, is a series of radiographs used to examine the gastrointestinal tract for abnormalities. A contrast medium, usually a radiocontrast agent such as barium sulfate mixed with water, is ingested or instilled into the gastrointestinal tract, and X-rays are used to create radiographs of the regions of interest. The barium enhances the visibility of the relevant parts of the gastrointestinal tract by coating the inside wall of the tract and appearing white on the film. This in combination with other plain radiographs allows for the imaging of parts of the upper gastrointestinal tract such as the pharynx, larynx, esophagus, stomach, and small intestine such that the inside wall lining, size, shape, contour, and patency are visible to the examiner. With fluoroscopy, it is also possible to visualize the functional movement of examined organs such as swallowing, peristalsis, or sphincter closure. Depending on the organs to be examined, barium radiographs can be classified into "barium swallow", "barium meal", "barium follow-through", and "enteroclysis". To further enhance the quality of images, air or gas is sometimes introduced into the gastrointestinal tract in addition to barium, and this procedure is called double-contrast imaging. In this case the gas is referred to as the negative contrast medium. Traditionally the images produced with barium contrast are made with plain-film radiography, but computed tomography is also used in combination with barium contrast, in which case the procedure is called "CT enterography".

Abdominal pain, also known as a stomach ache, is a symptom associated with both non-serious and serious medical issues. Since the abdomen contains most of the body's vital organs, it can be an indicator of a wide variety of diseases. Given that, approaching the examination of a person and planning of a differential diagnosis is extremely important.

Pyloric stenosis is a narrowing of the opening from the stomach to the first part of the small intestine. Symptoms include projectile vomiting without the presence of bile. This most often occurs after the baby is fed. The typical age that symptoms become obvious is two to twelve weeks old.

An omphalocele or omphalocoele, also known as an exomphalos, is a rare abdominal wall defect. Beginning at the 6th week of development, rapid elongation of the gut and increased liver size reduces intra abdominal space, which pushes intestinal loops out of the abdominal cavity. Around 10th week, the intestine returns to the abdominal cavity and the process is completed by the 12th week. Persistence of intestine or the presence of other abdominal viscera in the umbilical cord results in an omphalocele.
Enteric duplication cysts, sometimes simply called duplication cysts, are rare congenital malformations of the gastrointestinal tract. They most frequently occur in the small intestine, particularly the ileum, but can occur anywhere along the gastrointestinal tract. They may be cystic or tubular in conformation.

Gastroschisis is a birth defect in which the baby's intestines extend outside of the abdomen through a hole next to the belly button. The size of the hole is variable, and other organs including the stomach and liver may also occur outside the baby's body. Complications may include feeding problems, prematurity, intestinal atresia, and intrauterine growth restriction.

A volvulus is when a loop of intestine twists around itself and the mesentery that supports it, resulting in a bowel obstruction. Symptoms include abdominal pain, abdominal bloating, vomiting, constipation, and bloody stool. Onset of symptoms may be rapid or more gradual. The mesentery may become so tightly twisted that blood flow to part of the intestine is cut off, resulting in ischemic bowel. In this situation there may be fever or significant pain when the abdomen is touched.
Intestinal malrotation is a congenital anomaly of rotation of the midgut. It occurs during the first trimester as the fetal gut undergoes a complex series of growth and development. Malrotation can lead to a dangerous complication called volvulus, in which cases emergency surgery is indicated. Malrotation can refer to a spectrum of abnormal intestinal positioning, often including:

Annular pancreas is a rare condition in which the second part of the duodenum is surrounded by a ring of pancreatic tissue continuous with the head of the pancreas. This portion of the pancreas can constrict the duodenum and block or impair the flow of food to the rest of the intestines. It is estimated to occur in 1 out of 12,000 to 15,000 newborns. The ambiguity arises from the fact that not all cases are symptomatic.
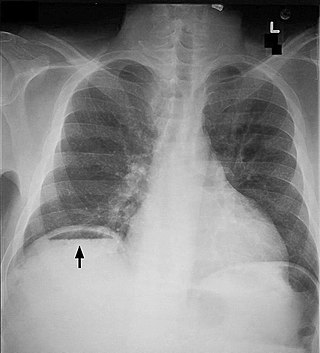
Pneumoperitoneum is pneumatosis in the peritoneal cavity, a potential space within the abdominal cavity. The most common cause is a perforated abdominal organ, generally from a perforated peptic ulcer, although any part of the bowel may perforate from a benign ulcer, tumor or abdominal trauma. A perforated appendix seldom causes a pneumoperitoneum.

The foregut in humans is the anterior part of the alimentary canal, from the distal esophagus to the first half of the duodenum, at the entrance of the bile duct. Beyond the stomach, the foregut is attached to the abdominal walls by mesentery. The foregut arises from the endoderm, developing from the folding primitive gut, and is developmentally distinct from the midgut and hindgut. Although the term “foregut” is typically used in reference to the anterior section of the primitive gut, components of the adult gut can also be described with this designation. Pain in the epigastric region, just below the intersection of the ribs, typically refers to structures in the adult foregut.

Distal intestinal obstruction syndrome (DIOS) involves obstruction of the distal part of the small intestines by thickened intestinal content and occurs in about 20% of mainly adult individuals with cystic fibrosis. DIOS was previously known as meconium ileus equivalent, a name which highlights its similarity to the intestinal obstruction seen in newborn infants with cystic fibrosis. DIOS tends to occur in older individuals with pancreatic insufficiency. Individuals with DIOS may be predisposed to bowel obstruction, though it is a separate entity than true constipation.

Intestinal atresia is any congenital malformation of the structure of the intestine that causes bowel obstruction. The malformation can be a narrowing (stenosis), absence or malrotation of a portion of the intestine. These defects can either occur in the small or large intestine.
Hematocolpos is a medical condition in which the vagina is pooled with menstrual blood due to multiple factors leading to the blockage of menstrual blood flow. The medical definition of hematocolpos is "an accumulation of blood within the vagina". It is often caused by the combination of menstruation with an imperforate hymen. It is sometimes seen in Robinow syndrome, uterus didelphys, or other vaginal anomalies.
Duodenal atresia is the congenital absence or complete closure of a portion of the lumen of the duodenum. It causes increased levels of amniotic fluid during pregnancy (polyhydramnios) and intestinal obstruction in newborn babies. Newborns present with bilious or non-bilous vomiting within the first 24 to 48 hours after birth, typically after their first oral feeding. Radiography shows a distended stomach and distended duodenum, which are separated by the pyloric valve, a finding described as the double-bubble sign.

Congenital pulmonary airway malformation (CPAM), formerly known as congenital cystic adenomatoid malformation (CCAM), is a congenital disorder of the lung similar to bronchopulmonary sequestration. In CPAM, usually an entire lobe of lung is replaced by a non-working cystic piece of abnormal lung tissue. This abnormal tissue will never function as normal lung tissue. The underlying cause for CPAM is unknown. It occurs in approximately 1 in every 30,000 pregnancies.
Neonatal bowel obstruction (NBO) or neonatal intestinal obstruction is the most common surgical emergency in the neonatal period. It may occur due to a variety of conditions and has an excellent outcome based on timely diagnosis and appropriate intervention.
