| Medial pontine syndrome | |
|---|---|
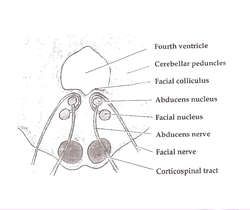 | |
| Pons. (Medial pontine syndrome affects structures at the bottom of the diagram: the corticospinal tract, abducens nerve, and occasionally the facial nerve. Medial lemniscus is also affected, but not pictured.) | |
| Specialty | Neurology |
Medial pontine syndrome or medial inferior pontine syndrome is a condition associated with a contralateral hemiplegia.[ citation needed ]"Medial inferior pontine syndrome" has been described as equivalent to Foville's syndrome. [1]
