Related Research Articles

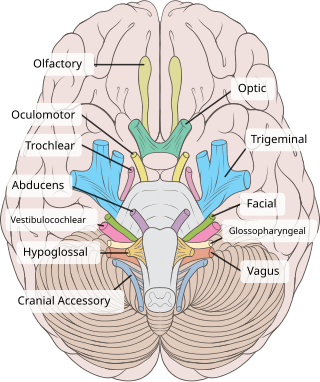
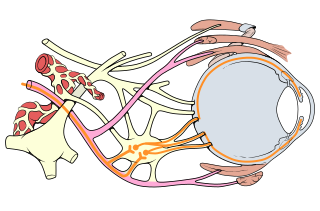
Cranial nerves are the nerves that emerge directly from the brain, of which there are conventionally considered twelve pairs. Cranial nerves relay information between the brain and parts of the body, primarily to and from regions of the head and neck, including the special senses of vision, taste, smell, and hearing.
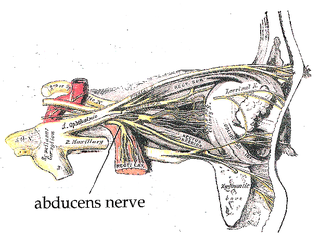
The abducens nerve or abducent nerve, also known as the sixth cranial nerve, cranial nerve VI, or simply CN VI, is a cranial nerve in humans and various other animals that controls the movement of the lateral rectus muscle, one of the extraocular muscles responsible for outward gaze. It is a somatic efferent nerve.

The facial nerve, also known as the seventh cranial nerve, cranial nerve VII, or simply CN VII, is a cranial nerve that emerges from the pons of the brainstem, controls the muscles of facial expression, and functions in the conveyance of taste sensations from the anterior two-thirds of the tongue. The nerve typically travels from the pons through the facial canal in the temporal bone and exits the skull at the stylomastoid foramen. It arises from the brainstem from an area posterior to the cranial nerve VI and anterior to cranial nerve VIII.
The oculomotor nerve, also known as the third cranial nerve, cranial nerve III, or simply CN III, is a cranial nerve that enters the orbit through the superior orbital fissure and innervates extraocular muscles that enable most movements of the eye and that raise the eyelid. The nerve also contains fibers that innervate the intrinsic eye muscles that enable pupillary constriction and accommodation. The oculomotor nerve is derived from the basal plate of the embryonic midbrain. Cranial nerves IV and VI also participate in control of eye movement.
The trochlear nerve, also known as the fourth cranial nerve, cranial nerve IV, or CN IV, is a cranial nerve that innervates a single muscle - the superior oblique muscle of the eye. Unlike most other cranial nerves, the trochlear nerve is exclusively a motor nerve.
The superior oblique muscle, or obliquus oculi superior, is a fusiform muscle originating in the upper, medial side of the orbit which abducts, depresses and internally rotates the eye. It is the only extraocular muscle innervated by the trochlear nerve.
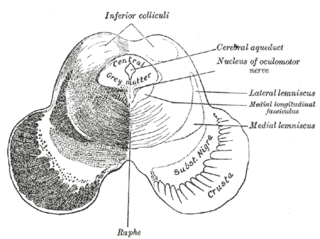
The medial longitudinal fasciculus (MLF) is an area of crossed over tracts, on each side of the brainstem. These bundles of axons are situated near the midline of the brainstem. They are made up of both ascending and descending fibers that arise from a number of sources and terminate in different areas, including the superior colliculus, the vestibular nuclei, and the cerebellum. It contains the interstitial nucleus of Cajal, responsible for oculomotor control, head posture, and vertical eye movement.

Diplopia is the simultaneous perception of two images of a single object that may be displaced horizontally or vertically in relation to each other. Also called double vision, it is a loss of visual focus under regular conditions, and is often voluntary. However, when occurring involuntarily, it results in impaired function of the extraocular muscles, where both eyes are still functional, but they cannot turn to target the desired object. Problems with these muscles may be due to mechanical problems, disorders of the neuromuscular junction, disorders of the cranial nerves that innervate the muscles, and occasionally disorders involving the supranuclear oculomotor pathways or ingestion of toxins.

Eye movement includes the voluntary or involuntary movement of the eyes. Eye movements are used by a number of organisms to fixate, inspect and track visual objects of interests. A special type of eye movement, rapid eye movement, occurs during REM sleep.
The inferior oblique muscle or obliquus oculi inferior is a thin, narrow muscle placed near the anterior margin of the floor of the orbit. The inferior oblique is one of the extraocular muscles, and is attached to the maxillary bone (origin) and the posterior, inferior, lateral surface of the eye (insertion). The inferior oblique is innervated by the inferior branch of the oculomotor nerve.

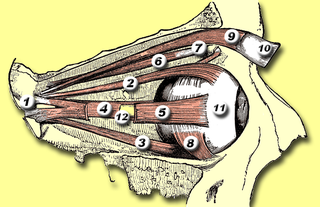
The extraocular muscles, or extrinsic ocular muscles, are the seven extrinsic muscles of the human eye. Six of the extraocular muscles, the four recti muscles, and the superior and inferior oblique muscles, control movement of the eye and the other muscle, the levator palpebrae superioris, controls eyelid elevation. The actions of the six muscles responsible for eye movement depend on the position of the eye at the time of muscle contraction.

Sixth nerve palsy, or abducens nerve palsy, is a disorder associated with dysfunction of cranial nerve VI, which is responsible for causing contraction of the lateral rectus muscle to abduct the eye. The inability of an eye to turn outward, results in a convergent strabismus or esotropia of which the primary symptom is diplopia in which the two images appear side-by-side. Thus, the diplopia is horizontal and worse in the distance. Diplopia is also increased on looking to the affected side and is partly caused by overaction of the medial rectus on the unaffected side as it tries to provide the extra innervation to the affected lateral rectus. These two muscles are synergists or "yoke muscles" as both attempt to move the eye over to the left or right. The condition is commonly unilateral but can also occur bilaterally.

Congenital fourth nerve palsy is a condition present at birth characterized by a vertical misalignment of the eyes due to a weakness or paralysis of the superior oblique muscle.

Hypertropia is a condition of misalignment of the eyes (strabismus), whereby the visual axis of one eye is higher than the fellow fixating eye. Hypotropia is the similar condition, focus being on the eye with the visual axis lower than the fellow fixating eye. Dissociated vertical deviation is a special type of hypertropia leading to slow upward drift of one or rarely both eyes, usually when the patient is inattentive.

Strabismus surgery is surgery on the extraocular muscles to correct strabismus, the misalignment of the eyes. Strabismus surgery is a one-day procedure that is usually performed under general anesthesia most commonly by either a neuro- or pediatric ophthalmologist. The patient spends only a few hours in the hospital with minimal preoperative preparation. After surgery, the patient should expect soreness and redness but is generally free to return home.
Fourth cranial nerve palsy or trochlear nerve palsy, is a condition affecting cranial nerve 4 (IV), the trochlear nerve, which is one of the cranial nerves. It causes weakness or paralysis of the superior oblique muscle that it innervates. This condition often causes vertical or near vertical double vision as the weakened muscle prevents the eyes from moving in the same direction together.
Brown syndrome is a rare form of strabismus characterized by limited elevation of the affected eye. The disorder may be congenital, or acquired. Brown syndrome is caused by a malfunction of the superior oblique muscle, causing the eye to have difficulty moving up, particularly during adduction. Harold W. Brown first described the disorder in 1950 and initially named it the "superior oblique tendon sheath syndrome".
Oculomotor nerve palsy or oculomotor neuropathy is an eye condition resulting from damage to the third cranial nerve or a branch thereof. As the name suggests, the oculomotor nerve supplies the majority of the muscles controlling eye movements. Damage to this nerve will result in an inability to move the eye normally. The nerve also supplies the upper eyelid muscle and is accompanied by parasympathetic fibers innervating the muscles responsible for pupil constriction. The limitations of eye movement resulting from the condition are generally so severe that patients are often unable to maintain normal eye alignment when gazing straight ahead, leading to strabismus and, as a consequence, double vision (diplopia).
Cyclotropia is a form of strabismus in which, compared to the correct positioning of the eyes, there is a torsion of one eye about the eye's visual axis. Consequently, the visual fields of the two eyes appear tilted relative to each other. The corresponding latent condition – a condition in which torsion occurs only in the absence of appropriate visual stimuli – is called cyclophoria.
The Parks–Bielschowsky three-step test, also known as Park's three-step test or Bielschowsky head tilt test, is a method used to isolate the paretic extraocular muscle, particularly superior oblique muscle and trochlear nerve, in acquired vertical double vision. It was originally described by Marshall M. Parks.
References
- Metz H, Lerner H: The adjustable Harada–Ito procedure. Arch Ophthalmol 1981;99 .
- Nishimura JK, Rosenbaum AL (2002). "The long-term torsion effect of the adjustable Harada-Ito procedure". J AAPOS. 6 (3): 141–4. doi:10.1067/mpa.2002.123429. PMID 12075289.