Related Research Articles
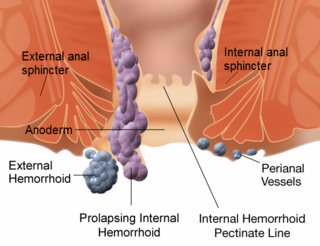
Hemorrhoids, also known as piles, are vascular structures in the anal canal. In their normal state, they are cushions that help with stool control. They become a disease when swollen or inflamed; the unqualified term "hemorrhoid" is often used to refer to the disease. The signs and symptoms of hemorrhoids depend on the type present. Internal hemorrhoids often result in painless, bright red rectal bleeding when defecating. External hemorrhoids often result in pain and swelling in the area of the anus. If bleeding occurs, it is usually darker. Symptoms frequently get better after a few days. A skin tag may remain after the healing of an external hemorrhoid.

Fecal incontinence (FI), or in some forms encopresis, is a lack of control over defecation, leading to involuntary loss of bowel contents, both liquid stool elements and mucus, or solid feces. When this loss includes flatus (gas), it is referred to as anal incontinence. FI is a sign or a symptom, not a diagnosis. Incontinence can result from different causes and might occur with either constipation or diarrhea. Continence is maintained by several interrelated factors, including the anal sampling mechanism, and incontinence usually results from deficiency of multiple mechanisms. The most common causes are thought to be immediate or delayed damage from childbirth, complications from prior anorectal surgery, altered bowel habits, and receptive anal sex. An estimated 2.2% of community dwelling adults are affected. However, reported prevalence figures vary. A prevalence of 8.39% among non-institutionalized U.S adults between 2005 and 2010 has been reported, and among institutionalized elders figures come close to 50%.
A fistula in anatomy is an abnormal connection between two hollow spaces, such as blood vessels, intestines, or other hollow organs. Types of fistula can be described by their location. Anal fistulas connect between the anal canal and the perianal skin. Anovaginal or rectovaginal fistulas occur when a hole develops between the anus or rectum and the vagina. Colovaginal fistulas occur between the colon and the vagina. Urinary tract fistulas are abnormal openings within the urinary tract or an abnormal connection between the urinary tract and another organ such as between the bladder and the uterus in a vesicouterine fistula, between the bladder and the vagina in a vesicovaginal fistula, and between the urethra and the vagina in urethrovaginal fistula. When occurring between two parts of the intestine, it is known as an enteroenteral fistula, between the small intestine and the skin as an enterocutaneous fistula, and between the colon and the skin as a colocutaneous fistula.

A rectal prolapse occurs when walls of the rectum have prolapsed to such a degree that they protrude out of the anus and are visible outside the body. However, most researchers agree that there are 3 to 5 different types of rectal prolapse, depending on whether the prolapsed section is visible externally, and whether the full or only partial thickness of the rectal wall is involved.

A rectovaginal fistula is a medical condition where there is a fistula or abnormal connection between the rectum and the vagina.
Colorectal surgery is a field in medicine dealing with disorders of the rectum, anus, and colon. The field is also known as proctology, but this term is now used infrequently within medicine and is most often employed to identify practices relating to the anus and rectum in particular. The word proctology is derived from the Greek words πρωκτός proktos, meaning "anus" or "hindparts", and -λογία -logia, meaning "science" or "study".

A colostomy is an opening (stoma) in the large intestine (colon), or the surgical procedure that creates one. The opening is formed by drawing the healthy end of the colon through an incision in the anterior abdominal wall and suturing it into place. This opening, often in conjunction with an attached ostomy system, provides an alternative channel for feces to leave the body. Thus if the natural anus is unavailable for that function, an artificial anus takes over. It may be reversible or irreversible, depending on the circumstances.

Ileostomy is a stoma constructed by bringing the end or loop of small intestine out onto the surface of the skin, or the surgical procedure which creates this opening. Intestinal waste passes out of the ileostomy and is collected in an external ostomy system which is placed next to the opening. Ileostomies are usually sited above the groin on the right hand side of the abdomen.
In medicine, the ileal pouch–anal anastomosis (IPAA), also known as an ileo-anal pouch, restorative proctocolectomy, ileal-anal pullthrough, or sometimes referred to as a j-pouch, s-pouch, w-pouch or an internal pouch, is an anastomosis of the ileum to the anus, bypassing the former site of the colon in cases where the colon has been removed. It retains or restores functionality of the anus, with stools passed under voluntary control of the patient, preventing fecal incontinence and serving as an alternative to ileostomy. The pouch component is a surgically constructed intestinal reservoir; usually situated near where the rectum would normally be. It is formed by folding loops of small intestine back on themselves and stitching or stapling them together. The internal walls are then removed thus forming a reservoir. The reservoir is then stitched or stapled into the perineum where the rectum was.

An imperforate anus or anorectal malformations (ARMs) are birth defects in which the rectum is malformed. ARMs are a spectrum of different congenital anomalies which vary from fairly minor lesions to complex anomalies. The cause of ARMs is unknown; the genetic basis of these anomalies is very complex because of their anatomical variability. In 8% of patients, genetic factors are clearly associated with ARMs. Anorectal malformation in Currarino syndrome represents the only association for which the gene HLXB9 has been identified.

Anal fistula is a chronic abnormal communication between the epithelialised surface of the anal canal and usually the perianal skin. An anal fistula can be described as a narrow tunnel with its internal opening in the anal canal and its external opening in the skin near the anus. Anal fistulae commonly occur in people with a history of anal abscesses. They can form when anal abscesses do not heal properly.

An anoscopy is an examination using a small, rigid, tubular instrument called an anoscope. This is inserted a few inches into the anus in order to evaluate problems of the anal canal. Anoscopy is used to diagnose hemorrhoids, anal fissures, and some cancers.

Anorectal abscess is an abscess adjacent to the anus. Most cases of perianal abscesses are sporadic, though there are certain situations which elevate the risk for developing the disease, such as diabetes mellitus, Crohn's disease, chronic corticosteroid treatment and others. It arises as a complication of paraproctitis. Ischiorectal, inter- and intrasphincteric abscesses have been described.
Pruritus ani is the irritation of the skin at the exit of the rectum, known as the anus, causing the desire to scratch. The intensity of anal itching increases from moisture, pressure, and rubbing caused by clothing and sitting. At worst, anal itching causes intolerable discomfort that often is accompanied by burning and soreness. It is estimated that up to 5% of the population of the United States experiences this type of discomfort daily.

The rectum is the final straight portion of the large intestine in humans and some other mammals, and the gut in others. The adult human rectum is about 12 centimetres (4.7 in) long, and begins at the rectosigmoid junction at the level of the third sacral vertebra or the sacral promontory depending upon what definition is used. Its diameter is similar to that of the sigmoid colon at its commencement, but it is dilated near its termination, forming the rectal ampulla. It terminates at the level of the anorectal ring or the dentate line, again depending upon which definition is used. In humans, the rectum is followed by the anal canal which is about 4 centimetres (1.6 in) long, before the gastrointestinal tract terminates at the anal verge. The word rectum comes from the Latin rectumintestinum, meaning straight intestine.

In humans, the anus is the external opening of the rectum, located inside the intergluteal cleft and separated from the genitals by the perineum. Two sphincters control the exit of feces from the body during an act of defecation, which is the primary function of the anus. These are the internal anal sphincter and the external anal sphincter, which are circular muscles that normally maintain constriction of the orifice and which relaxes as required by normal physiological functioning. The inner sphincter is involuntary and the outer is voluntary. It is located behind the perineum which is located behind the vagina or scrotum.
Rectal discharge is intermittent or continuous expression of liquid from the anus. Normal rectal mucus is needed for proper excretion of waste. Otherwise, this is closely related to types of fecal incontinence but the term rectal discharge does not necessarily imply degrees of incontinence. Types of fecal incontinence that produce a liquid leakage could be thought of as a type of rectal discharge.

Anorectal disorders include conditions involving the anorectal junction as seen in the image. They are painful but common conditions like hemorrhoids, tears, fistulas, or abscesses that affect the anal region. Most people experience some form of anorectal disorder during their lifetime. Primary care physicians can treat most of these disorders, however, high-risk individuals include those with HIV, roughly half of whom need surgery to remedy the disorders. Likelihood of malignancy should also be considered in high risk individuals. This is why it is important to perform a full history and physical exam on each patient. Because these disorders affect the rectum, people are often embarrassed or afraid to confer with a medical professional.
Warren operation is a surgery performed to correct anal incontinence. It is done by disrupting the anterior segment of the anal sphincter, perineal body and rectovaginal septum.
A urogenital fistula is an abnormal tract that exists between the urinary tract and bladder, ureters, or urethra. A urogenital fistula can occur between any of the organs and structures of the pelvic region. A fistula allows urine to continually exit through and out the urogenital tract. This can result in significant disability, interference with sexual activity, and other physical health issues, the effects of which may in turn have a negative impact on mental or emotional state, including an increase in social isolation. Urogenital fistulas vary in etiology. Fistulas are usually caused by injury or surgery, but they can also result from malignancy, infection, prolonged and obstructed labor and deliver in childbirth, hysterectomy, radiation therapy or inflammation. Of the fistulas that develop from difficult childbirth, 97 percent occur in developing countries. Congenital urogenital fistulas are rare; only ten cases have been documented. Abnormal passageways can also exist between the vagina and the organs of the gastrointestinal system, and these may also be termed fistulas.
References
- 1 2 3 4 Corman, Marvin L. (2005). Colon and Rectal Surgery. Lippincott Williams & Wilkins. pp. 575–576. ISBN 9780781740432.
- 1 2 3 4 5 Puri, Prem (2003). Newborn Surgery (2nd ed.). CRC Press. p. 539. ISBN 9780340761441.
- 1 2 3 4 Rintala, Risto J. (2005). "Congenital anorectal anomalies". Paediatric Surgery (2nd ed.). CRC Press. pp. 157–158. ISBN 9780340809105.
- 1 2 Browne, Nancy Tkacz (2008). Nursing Care of the Pediatric Surgical Patient. Jones & Bartlett Learning. p. 305. ISBN 9780763768034.
- 1 2 Mattei, Peter (2011). Fundamentals of Pediatric Surgery. Springer Science+Business Media. p. 500. ISBN 9781441966438.