
The trachea, also known as the windpipe, is a cartilaginous tube that connects the larynx to the bronchi of the lungs, allowing the passage of air, and so is present in almost all animals lungs. The trachea extends from the larynx and branches into the two primary bronchi. At the top of the trachea, the cricoid cartilage attaches it to the larynx. The trachea is formed by a number of horseshoe-shaped rings, joined together vertically by overlying ligaments, and by the trachealis muscle at their ends. The epiglottis closes the opening to the larynx during swallowing.

The esophagus, oesophagus, or œsophagus all ; pl.: ( e)(œ)sophagi or (œ)sophaguses), colloquially known also as the food pipe, food tube, or gullet, is an organ in vertebrates through which food passes, aided by peristaltic contractions, from the pharynx to the stomach. The esophagus is a fibromuscular tube, about 25 cm (10 in) long in adults, that travels behind the trachea and heart, passes through the diaphragm, and empties into the uppermost region of the stomach. During swallowing, the epiglottis tilts backwards to prevent food from going down the larynx and lungs. The word oesophagus is from Ancient Greek οἰσοφάγος (oisophágos), from οἴσω (oísō), future form of φέρω + ἔφαγον.
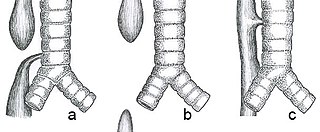
Esophageal atresia is a congenital medical condition that affects the alimentary tract. It causes the esophagus to end in a blind-ended pouch rather than connecting normally to the stomach. It comprises a variety of congenital anatomic defects that are caused by an abnormal embryological development of the esophagus. It is characterized anatomically by a congenital obstruction of the esophagus with interruption of the continuity of the esophageal wall.
Tracheomalacia is a condition or incident where the cartilage that keeps the airway (trachea) open is soft such that the trachea partly collapses especially during increased airflow. This condition is most commonly seen in infants and young children. The usual symptom is stridor when a person breathes out. This is usually known as a collapsed windpipe.

Esophagitis, also spelled oesophagitis, is a disease characterized by inflammation of the esophagus. The esophagus is a tube composed of a mucosal lining, and longitudinal and circular smooth muscle fibers. It connects the pharynx to the stomach; swallowed food and liquids normally pass through it.
In anatomy, a fistula is an abnormal connection joining two hollow spaces, such as blood vessels, intestines, or other hollow organs to each other, often resulting in an abnormal flow of fluid from one space to the other. An anal fistula connects the anal canal to the perianal skin. An anovaginal or rectovaginal fistula is a hole joining the anus or rectum to the vagina. A colovaginal fistula joins the space in the colon to that in the vagina. A urinary tract fistula is an abnormal opening in the urinary tract or an abnormal connection between the urinary tract and another organ. An abnormal communication between the bladder and the uterus is called a vesicouterine fistula, while if it is between the bladder and the vagina it is known as a vesicovaginal fistula, and if between the urethra and the vagina: a urethrovaginal fistula. When occurring between two parts of the intestine, it is known as an enteroenteral fistula, between the small intestine and the skin it's known as an enterocutaneous fistula, and between the colon and the skin as a colocutaneous fistula.

A feeding tube is a medical device used to provide nutrition to people who cannot obtain nutrition by mouth, are unable to swallow safely, or need nutritional supplementation. The state of being fed by a feeding tube is called gavage, enteral feeding or tube feeding. Placement may be temporary for the treatment of acute conditions or lifelong in the case of chronic disabilities. A variety of feeding tubes are used in medical practice. They are usually made of polyurethane or silicone. The outer diameter of a feeding tube is measured in French units. They are classified by the site of insertion and intended use.

Laryngectomy is the removal of the larynx. In a total laryngectomy, the entire larynx is removed with the separation of the airway from the mouth, nose and esophagus. In a partial laryngectomy, only a portion of the larynx is removed. Following the procedure, the person breathes through an opening in the neck known as a stoma. This procedure is usually performed by an ENT surgeon in cases of laryngeal cancer. Many cases of laryngeal cancer are treated with more conservative methods. A laryngectomy is performed when these treatments fail to conserve the larynx or when the cancer has progressed such that normal functioning would be prevented. Laryngectomies are also performed on individuals with other types of head and neck cancer. Less invasive partial laryngectomies, including tracheal shaves and feminization laryngoplasty may also be performed on transgender women and other female or non-binary identified individuals to feminize the larynx and/or voice. Post-laryngectomy rehabilitation includes voice restoration, oral feeding and more recently, smell and taste rehabilitation. An individual's quality of life can be affected post-surgery.

Pediatric surgery is a subspecialty of surgery involving the surgery of fetuses, infants, children, adolescents, and young adults.
Atresia is a condition in which an orifice or passage in the body is closed or absent.

The VACTERL association refers to a recognized group of birth defects which tend to co-occur. This pattern is a recognized association, as opposed to a syndrome, because there is no known pathogenetic cause to explain the grouped incidence.
A vascular ring is a congenital defect in which there is an abnormal formation of the aorta and/or its surrounding blood vessels. The trachea and esophagus are completely encircled and sometimes compressed by a "ring" formed by these vessels, which can lead to breathing and digestive difficulties.
The tracheoesophageal septum is an embryological structure. It is formed from the tracheoesophageal folds or ridges which fuse in the midline. It divides the oesophagus from the trachea during prenatal development. Developmental abnormalities can lead to a tracheoesophageal fistula.
A tracheo-esophageal puncture is a surgically created hole between the trachea (windpipe) and the esophagus in a person who has had a total laryngectomy, a surgery where the larynx is removed. The purpose of the puncture is to restore a person’s ability to speak after the vocal cords have been removed. This involves creation of a fistula between the trachea and the esophagus, puncturing the short segment of tissue or “common wall” that typically separates these two structures. A voice prosthesis is inserted into this puncture. The prosthesis keeps food out of the trachea but lets air into the esophagus for esophageal speech.

Bronchomalacia is a term for weak cartilage in the walls of the bronchial tubes, often occurring in children under a day. Bronchomalacia means 'floppiness' of some part of the bronchi. Patients present with noisy breathing and/or wheezing. There is collapse of a main stem bronchus on exhalation. If the trachea is also involved the term tracheobronchomalacia (TBM) is used. If only the upper airway the trachea is involved it is called tracheomalacia (TM). There are two types of bronchomalacia. Primary bronchomalacia is due to a deficiency in the cartilaginous rings. Secondary bronchomalacia may occur by extrinsic compression from an enlarged vessel, a vascular ring or a bronchogenic cyst. Though uncommon, idiopathic tracheobronchomalacia has been described in older adults.

Esophageal diseases can derive from congenital conditions, or they can be acquired later in life.
Double aortic arch is a relatively rare congenital cardiovascular malformation. DAA is an anomaly of the aortic arch in which two aortic arches form a complete vascular ring that can compress the trachea and/or esophagus. Most commonly there is a larger (dominant) right arch behind and a smaller (hypoplastic) left aortic arch in front of the trachea/esophagus. The two arches join to form the descending aorta which is usually on the left side. In some cases the end of the smaller left aortic arch closes and the vascular tissue becomes a fibrous cord. Although in these cases a complete ring of two patent aortic arches is not present, the term ‘vascular ring’ is the accepted generic term even in these anomalies.
A laryngeal cleft or laryngotracheoesophageal cleft is a rare congenital abnormality in the posterior laryngo-tracheal wall. It occurs in approximately 1 in 10,000 to 20,000 births. It means there is a communication between the oesophagus and the trachea, which allows food or fluid to pass into the airway.
Tracheal agenesis is a rare birth defect with a prevalence of less than 1 in 50,000 in which the trachea fails to develop, resulting in an impaired communication between the larynx and the alveoli of the lungs. Although the defect is normally fatal, occasional cases have been reported of long-term survival following surgical intervention.

Mandibulofacial dysostosis with microcephaly syndrome, also known as growth delay-intellectual disability-mandibulofacial dysostosis-microcephaly-cleft palate syndrome, mandibulofacial dysostosis, guion-almeida type, or simply as MFDM syndrome is a rare genetic disorder which is characterized by developmental delays, intellectual disabilities, and craniofacial dysmorphisms.

