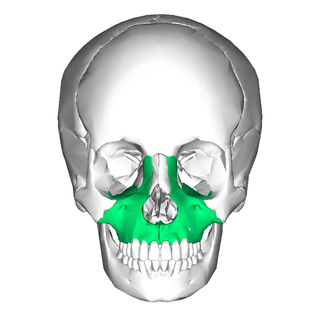
In vertebrates, the maxilla is the upper fixed bone of the jaw formed from the fusion of two maxillary bones. In humans, the upper jaw includes the hard palate in the front of the mouth. The two maxillary bones are fused at the intermaxillary suture, forming the anterior nasal spine. This is similar to the mandible, which is also a fusion of two mandibular bones at the mandibular symphysis. The mandible is the movable part of the jaw.

In the human skull, the zygomatic bone, also called cheekbone or malar bone, is a paired irregular bone, situated at the upper and lateral part of the face and forming part of the lateral wall and floor of the orbit, of the temporal fossa and the infratemporal fossa. It presents a malar and a temporal surface; four processes, and four borders.

In anatomy, the palatine bones are two irregular bones of the facial skeleton in many animal species, located above the uvula in the throat. Together with the maxilla, they comprise the hard palate.

The temporal bones are situated at the sides and base of the skull, and lateral to the temporal lobes of the cerebral cortex.

In anatomy, the zygomatic arch, or cheek bone, is a part of the skull formed by the zygomatic process of the temporal bone and the temporal process of the zygomatic bone, the two being united by an oblique suture ; the tendon of the temporal muscle passes medial to the arch, to gain insertion into the coronoid process of the mandible (jawbone).

In anatomy, the orbit is the cavity or socket/hole of the skull in which the eye and its appendages are situated. "Orbit" can refer to the bony socket, or it can also be used to imply the contents. In the adult human, the volume of the orbit is 30 millilitres, of which the eye occupies 6.5 ml. The orbital contents comprise the eye, the orbital and retrobulbar fascia, extraocular muscles, cranial nerves II, III, IV, V, and VI, blood vessels, fat, the lacrimal gland with its sac and duct, the eyelids, medial and lateral palpebral ligaments, cheek ligaments, the suspensory ligament, septum, ciliary ganglion and short ciliary nerves.

The pyramid-shaped maxillary sinus is the largest of the paranasal sinuses, located in the maxilla. It drains into the middle meatus of the nose through the semilunar hiatus. It is located to the side of the nasal cavity, and below the orbit.

The temporal fossa is a fossa on the side of the skull bounded by the temporal lines above, and the zygomatic arch below. Its floor is formed by the outer surfaces of four bones of the skull. The fossa is filled by the temporalis muscle.

In neuroanatomy, the maxillary nerve (V2) is one of the three branches or divisions of the trigeminal nerve, the fifth (CN V) cranial nerve. It comprises the principal functions of sensation from the maxilla, nasal cavity, sinuses, the palate and subsequently that of the mid-face, and is intermediate, both in position and size, between the ophthalmic nerve and the mandibular nerve.

The zygomatic nerve is a branch of the maxillary nerve. It arises in the pterygopalatine fossa and enters the orbit through the inferior orbital fissure before dividing into its two terminal branches: the zygomaticotemporal nerve and zygomaticofacial nerve.
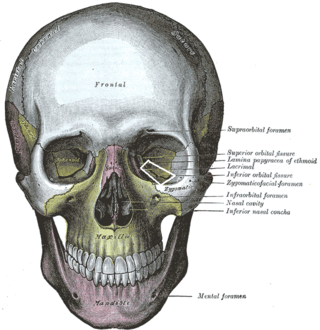
The inferior orbital fissure is a gap between the greater wing of sphenoid bone, and the maxilla. It connects the orbit (anteriorly) with the infratemporal fossa and pterygopalatine fossa (posteriorly).
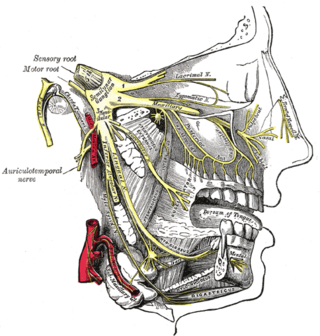
The zygomaticotemporal nerve (zygomaticotemporal branch, temporal branch) is a cutaneous (sensory) nerve of the head. It is a branch of the zygomatic nerve (itself a branch of the maxillary nerve (CN V2)). It arises in the orbit and exits the orbit through the zygomaticotemporal foramen in the zygomatic bone to enter the temporal fossa. It is distributed to the skin of the side of the forehead. It also contains a parasympathetic secretomotor component for the lacrimal gland which it confers to the lacrimal nerve (which then delivers it to the gland).

The infratemporal fossa is an irregularly shaped cavity that is a part of the skull. It is situated below and medial to the zygomatic arch. It is not fully enclosed by bone in all directions. It contains superficial muscles, including the lower part of the temporalis muscle, the lateral pterygoid muscle, and the medial pterygoid muscle. It also contains important blood vessels such as the middle meningeal artery, the pterygoid plexus, and the retromandibular vein, and nerves such as the mandibular nerve (CN V3) and its branches.

The zygomatic processes are three processes (protrusions) from other bones of the skull which each articulate with the zygomatic bone. The three processes are:
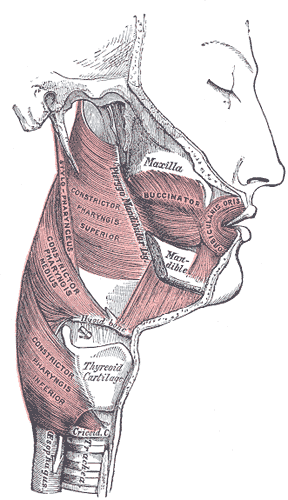
The buccal space is a fascial space of the head and neck. It is a potential space in the cheek, and is paired on each side. The buccal space is superficial to the buccinator muscle and deep to the platysma muscle and the skin. The buccal space is part of the subcutaneous space, which is continuous from head to toe.

An orbital blowout fracture is a traumatic deformity of the orbital floor or medial wall that typically results from the impact of a blunt object larger than the orbital aperture, or eye socket. Most commonly this results in a herniation of orbital contents through the orbital fractures. The proximity of maxillary and ethmoidal sinus increases the susceptibility of the floor and medial wall for the orbital blowout fracture in these anatomical sites. Most commonly, the inferior orbital wall, or the floor, is likely to collapse, because the bones of the roof and lateral walls are robust. Although the bone forming the medial wall is the thinnest, it is buttressed by the bone separating the ethmoidal air cells. The comparatively thin bone of the floor of the orbit and roof of the maxillary sinus has no support and so the inferior wall collapses mostly. Therefore, medial wall blowout fractures are the second-most common, and superior wall, or roof and lateral wall, blowout fractures are uncommon and rare, respectively. They are characterized by double vision, sunken ocular globes, and loss of sensation of the cheek and upper gums from infraorbital nerve injury.

The Le Fortfractures are a pattern of midface fractures originally described by the French surgeon, René Le Fort, in the early 1900s. He described three distinct fracture patterns. Although not always applicable to modern-day facial fractures, the Le Fort type fracture classification is still utilized today by medical providers to aid in describing facial trauma for communication, documentation, and surgical planning. Several surgical techniques have been established for facial reconstruction following Le Fort fractures, including maxillomandibular fixation (MMF) and open reduction and internal fixation (ORIF). The main goal of any surgical intervention is to re-establish occlusion, or the alignment of upper and lower teeth, to ensure the patient is able to eat. Complications following Le Fort fractures rely on the anatomical structures affected by the inciding injury.
Zygoma reduction, also known as cheekbone reduction surgery, is a surgery used to reduce the facial width by excising part of the zygomatic bone and arch. Wide cheekbones are a characteristic facial trait of Asians, whose skull shapes tend to be more brachycephalic in comparison with Caucasian counterparts, whose skull shapes tend to be more dolichocephalic .This surgery is popular among Asians due to their inherent wide cheekbones. Due to the advanced surgical skills of Korean surgeons who perform facial contouring surgeries, the number of Asian people undergoing this surgery is increasing.
Caldwell-Luc surgery, Caldwell-Luc operation, also known as Caldwell-Luc antrostomy, and Radical antrostomy, is an operation to remove irreversibly damaged mucosa of the maxillary sinus. It is done when maxillary sinusitis is not cured by medication or other non-invasive technique. The approach is mainly from the anterior wall of the maxilla bone. It was introduced by George Caldwell (1893)and Henry Luc (1897). The maxillary sinus is entered from two separate openings, one in the canine fossa to gain access to the antrum and other in the naso antral wall for drainage.
A zygoma fracture is a form of facial fracture caused by a fracture of the zygomatic bone. Symptoms include flattening of the face, trismus and lateral subconjunctival hemorrhage.
