The clavicle, collarbone, or keybone is a slender, S-shaped long bone approximately 6 inches (15 cm) long that serves as a strut between the shoulder blade and the sternum (breastbone). There are two clavicles, one on the left and one on the right. The clavicle is the only long bone in the body that lies horizontally. Together with the shoulder blade, it makes up the shoulder girdle. It is a palpable bone and, in people who have less fat in this region, the location of the bone is clearly visible. It receives its name from Latin clavicula 'little key' because the bone rotates along its axis like a key when the shoulder is abducted. The clavicle is the most commonly fractured bone. It can easily be fractured by impacts to the shoulder from the force of falling on outstretched arms or by a direct hit.

The scapula, also known as the shoulder blade, is the bone that connects the humerus with the clavicle. Like their connected bones, the scapulae are paired, with each scapula on either side of the body being roughly a mirror image of the other. The name derives from the Classical Latin word for trowel or small shovel, which it was thought to resemble.

The coracoid process is a small hook-like structure on the lateral edge of the superior anterior portion of the scapula. Pointing laterally forward, it, together with the acromion, serves to stabilize the shoulder joint. It is palpable in the deltopectoral groove between the deltoid and pectoralis major muscles.

The brachiocephalic artery, brachiocephalic trunk, or innominate artery is an artery of the mediastinum that supplies blood to the right arm, head, and neck.

The human shoulder is made up of three bones: the clavicle (collarbone), the scapula, and the humerus as well as associated muscles, ligaments and tendons.

The ankle, the talocrural region or the jumping bone (informal) is the area where the foot and the leg meet. The ankle includes three joints: the ankle joint proper or talocrural joint, the subtalar joint, and the inferior tibiofibular joint. The movements produced at this joint are dorsiflexion and plantarflexion of the foot. In common usage, the term ankle refers exclusively to the ankle region. In medical terminology," can refer broadly to the region or specifically to the talocrural joint.

The upper limbs or upper extremities are the forelimbs of an upright-postured tetrapod vertebrate, extending from the scapulae and clavicles down to and including the digits, including all the musculatures and ligaments involved with the shoulder, elbow, wrist and knuckle joints. In humans, each upper limb is divided into the arm, forearm and hand, and is primarily used for climbing, lifting and manipulating objects.

The rhomboid major is a skeletal muscle of the back that connects the scapula with the vertebrae of the spinal column. It originates from the spinous processes of the thoracic vertebrae T2–T5 and supraspinous ligament; it inserts onto the lower portion of the medial border of the scapula. It acts together with the rhomboid minor to keep the scapula pressed against thoracic wall and to retract the scapula toward the vertebral column.
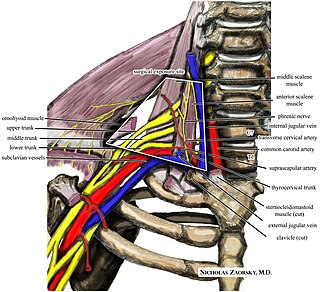
Thoracic outlet syndrome (TOS) is a condition in which there is compression of the nerves, arteries, or veins in the superior thoracic aperture, the passageway from the lower neck to the armpit, also known as the thoracic outlet. There are three main types: neurogenic, venous, and arterial. The neurogenic type is the most common and presents with pain, weakness, paraesthesia, and occasionally loss of muscle at the base of the thumb. The venous type results in swelling, pain, and possibly a bluish coloration of the arm. The arterial type results in pain, coldness, and pallor of the arm.
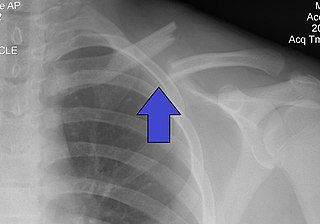
A clavicle fracture, also known as a broken collarbone, is a bone fracture of the clavicle. Symptoms typically include pain at the site of the break and a decreased ability to move the affected arm. Complications can include a collection of air in the pleural space surrounding the lung (pneumothorax), injury to the nerves or blood vessels in the area, and an unpleasant appearance.
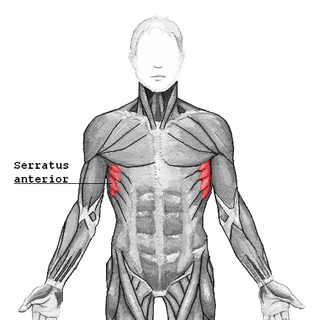
The serratus anterior is a muscle of the chest. It originates at the side of the chest from the upper 8 or 9 ribs; it inserts along the entire length of the anterior aspect of the medial border of the scapula. It is innervated by the long thoracic nerve from the brachial plexus. The serratus anterior acts to pull the scapula forward around the thorax.

The subclavius is a small triangular muscle, placed between the clavicle and the first rib. Along with the pectoralis major and pectoralis minor muscles, the subclavius muscle makes up the anterior axioappendicular muscles, also known as anterior wall of the axilla.
The shoulder girdle or pectoral girdle is the set of bones in the appendicular skeleton which connects to the arm on each side. In humans it consists of the clavicle and scapula; in those species with three bones in the shoulder, it consists of the clavicle, scapula, and coracoid. Some mammalian species have only the scapula.
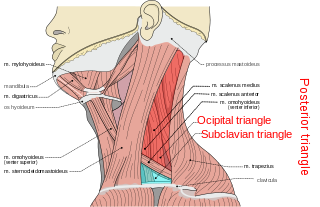
The posterior triangle is a region of the neck.

The suprascapular artery is a branch of the thyrocervical trunk on the neck.

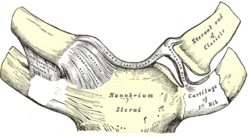
The coracoclavicular ligament is a ligament of the shoulder. It connects the clavicle to the coracoid process of the scapula.

The glenoid fossa of the scapula or the glenoid cavity is a bone part of the shoulder. The word glenoid is pronounced or and is from Greek: gléne, "socket", reflecting the shoulder joint's ball-and-socket form. It is a shallow, pyriform articular surface, which is located on the lateral angle of the scapula. It is directed laterally and forward and articulates with the head of the humerus; it is broader below than above and its vertical diameter is the longest.
The coracoacromial ligament is a strong triangular ligament between the coracoid process and the acromion. It protects the head of the humerus. Its acromial attachment may be repositioned to the clavicle during reconstructive surgery of the acromioclavicular joint.

A separated shoulder, also known as acromioclavicular joint injury, is a common injury to the acromioclavicular joint. The AC joint is located at the outer end of the clavicle where it attaches to the acromion of the scapula. Symptoms include non-radiating pain which may make it difficult to move the shoulder. The presence of swelling or bruising and a deformity in the shoulder is also common depending on how severe the dislocation is.
Glenolabral articular disruption (GLAD) lesion is a type of shoulder injury. It is difficult to diagnose clinically, and requires surgical repair to correct the damage to the shoulder.