
The ulna or ulnar bone is a long bone in the forearm stretching from the elbow to the wrist. It is on the same side of the forearm as the little finger, running parallel to the radius, the forearm's other long bone. Longer and thinner than the radius, the ulna is considered to be the smaller long bone of the lower arm. The corresponding bone in the lower leg is the fibula.

The humerus is a long bone in the arm that runs from the shoulder to the elbow. It connects the scapula and the two bones of the lower arm, the radius and ulna, and consists of three sections. The humeral upper extremity consists of a rounded head, a narrow neck, and two short processes. The body is cylindrical in its upper portion, and more prismatic below. The lower extremity consists of 2 epicondyles, 2 processes, and 3 fossae. As well as its true anatomical neck, the constriction below the greater and lesser tubercles of the humerus is referred to as its surgical neck due to its tendency to fracture, thus often becoming the focus of surgeons.
The forearm is the region of the upper limb between the elbow and the wrist. The term forearm is used in anatomy to distinguish it from the arm, a word which is used to describe the entire appendage of the upper limb, but which in anatomy, technically, means only the region of the upper arm, whereas the lower "arm" is called the forearm. It is homologous to the region of the leg that lies between the knee and the ankle joints, the crus.
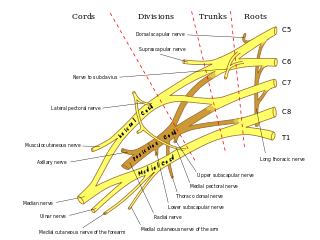
In human anatomy, the ulnar nerve is a nerve that runs near the ulna bone. The ulnar collateral ligament of elbow joint is in relation with the ulnar nerve. The nerve is the largest in the human body unprotected by muscle or bone, so injury is common. This nerve is directly connected to the little finger, and the adjacent half of the ring finger, innervating the palmar aspect of these fingers, including both front and back of the tips, perhaps as far back as the fingernail beds.

The radius or radial bone is one of the two large bones of the forearm, the other being the ulna. It extends from the lateral side of the elbow to the thumb side of the wrist and runs parallel to the ulna. The ulna is longer than the radius, but the radius is thicker. The radius is a long bone, prism-shaped and slightly curved longitudinally.
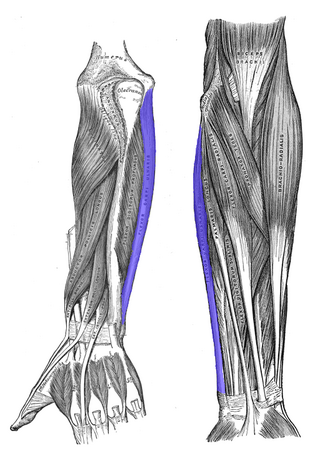
The flexor carpi ulnaris (FCU) is a muscle of the forearm that flexes and adducts at the wrist joint.

The olecranon, is a large, thick, curved bony process on the proximal, posterior end of the ulna. It forms the protruding part of the elbow and is opposite to the cubital fossa or elbow pit. The olecranon serves as a lever for the extensor muscles that straighten the elbow joint.
The pronator teres is a muscle that, along with the pronator quadratus, serves to pronate the forearm. It has two origins, at the medial humeral supracondylar ridge and the ulnar tuberosity, and inserts near the middle of the radius.
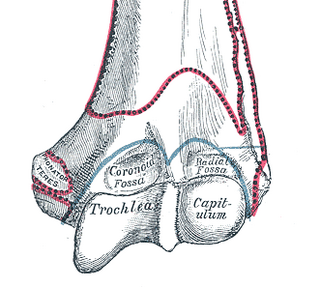
In the human arm, the humeral trochlea is the medial portion of the articular surface of the elbow joint which articulates with the trochlear notch on the ulna in the forearm.
The medial epicondyle of the humerus is an epicondyle of the humerus bone of the upper arm in humans. It is larger and more prominent than the lateral epicondyle and is directed slightly more posteriorly in the anatomical position. In birds, where the arm is somewhat rotated compared to other tetrapods, it is called the ventral epicondyle of the humerus. In comparative anatomy, the more neutral term entepicondyle is used.

The posterior ulnar recurrent artery is an artery in the forearm. It is one of two recurrent arteries that arises from the ulnar artery, the other being the anterior ulnar recurrent artery. The posterior ulnar recurrent artery being much larger than the anterior and also arises somewhat lower than it.

The radial collateral ligament (RCL), lateral collateral ligament (LCL), or external lateral ligament is a ligament in the elbow on the side of the radius.

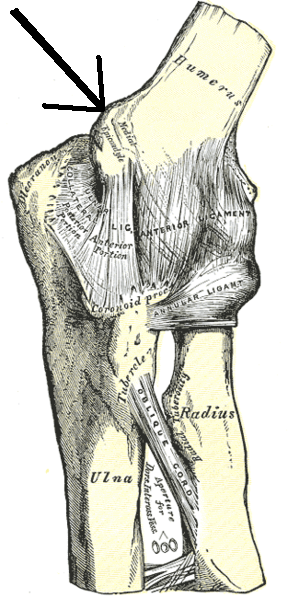
The anterior ligament of the elbow is a broad and thin fibrous layer covering the anterior surface of the joint.

The fascial compartments of arm refers to the specific anatomical term of the compartments within the upper segment of the upper limb of the body. The upper limb is divided into two segments, the arm and the forearm. Each of these segments is further divided into two compartments which are formed by deep fascia – tough connective tissue septa (walls). Each compartment encloses specific muscles and nerves.
The coronoid process of the ulna is a triangular process projecting forward from the anterior proximal portion of the ulna.
The humeroulnar joint is part of the elbow-joint. It is composed of two bones, the humerus and ulna, and is the junction between the trochlear notch of ulna and the trochlea of humerus. It is classified as a simple hinge-joint, which allows for movements of flexion, extension and circumduction. Owing to the obliquity of the trochlea of the humerus, this movement does not take place in the antero-posterior plane of the body of the humerus.

The elbow is the region between the upper arm and the forearm that surrounds the elbow joint. The elbow includes prominent landmarks such as the olecranon, the cubital fossa, and the lateral and the medial epicondyles of the humerus. The elbow joint is a hinge joint between the arm and the forearm; more specifically between the humerus in the upper arm and the radius and ulna in the forearm which allows the forearm and hand to be moved towards and away from the body. The term elbow is specifically used for humans and other primates, and in other vertebrates it is not used. In those cases, forelimb plus joint is used.

A supracondylar humerus fracture is a fracture of the distal humerus just above the elbow joint. The fracture is usually transverse or oblique and above the medial and lateral condyles and epicondyles. This fracture pattern is relatively rare in adults, but is the most common type of elbow fracture in children. In children, many of these fractures are non-displaced and can be treated with casting. Some are angulated or displaced and are best treated with surgery. In children, most of these fractures can be treated effectively with expectation for full recovery. Some of these injuries can be complicated by poor healing or by associated blood vessel or nerve injuries with serious complications.

The extrinsic extensor muscles of the hand are located in the back of the forearm and have long tendons connecting them to bones in the hand, where they exert their action. Extrinsic denotes their location outside the hand. Extensor denotes their action which is to extend, or open flat, joints in the hand. They include the extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), extensor digitorum (ED), extensor digiti minimi (EDM), extensor carpi ulnaris (ECU), abductor pollicis longus (APL), extensor pollicis brevis (EPB), extensor pollicis longus (EPL), and extensor indicis (EI).

Ulnar collateral ligament injuries can occur during certain activities such as overhead baseball pitching. Acute or chronic disruption of the ulnar collateral ligament result in medial elbow pain, valgus instability, and impaired throwing performance. There are both non-surgical and surgical treatment options.



