Model development
| | This section needs expansion. You can help by adding to it. (April 2012) |
Adapted categorical models
There are different ways to ‘dimensionalize’ personality disorders, these can be summarised into two categories.
- The first involves quantifying DSM-5 pathology. This can be done either based on the degree to which symptoms are present or on how close to a prototypic presentation a patient's presentation may be. The prototype approach includes features not present in the DSM. [18]
- The second approach involves identification of DSM disorder traits by means of factor analysis to show underlying dimensions of the personality disorder criteria, this method may also include relevant psychopathology. [17]
Normal personality models
Five-factor model
The Five-Factor model of personality, which is the most dominant dimensional model, [19] has been used to conceptualize personality disorders and has received various empirical support. Under this approach, extreme levels of the basic personality traits identified by the FFM are what contributes to the maladaptive nature of personality disorders. [20] Over 50 published studies supporting this model have been identified, providing much empirical support for this approach. Most of these studies examine the relationship between scores on separate measures of Big Five trait and personality disorder symptoms. [20]
The Five-Factor model was first extended to personality disorders in the early 1990s, when it was established that a satisfactory profile of each personality disorder in the DSM-III-R could be created through various levels of Big Five traits. [5] Thomas Widiger and his colleagues have demonstrated that many of the central elements of personality disorders can be explained in terms of Big Five traits – for example, borderline personality disorder is characterized by high levels of hostility, trait anxiety and depression, and vulnerability, all of which are facets of neuroticism. [5] This approach also helps to differentiate characteristics of disorders that overlap under the current categorical model, such as avoidant and schizoid personality disorders. The Five-Factor-based approach explains much of that overlap as well as the ways in which they are different. [5] For example, both are characterized primarily by maladaptive excessive introversion, but avoidant personality disorder also includes high levels of facets of neuroticism (such as self-consciousness, anxiety, and vulnerability), while schizotypal personality disorder includes the addition of low assertiveness. The Five-Factor approach also resolves previous anomalies in factor analyses of personality disorders, which makes it a more explanatory model than the current categorical approach, which only includes three factors (odd-eccentric, dramatic-emotional, and anxious-fearful). [5]
A prototype diagnostic technique has been developed in which Five-Factor-based prototypes for each disorder were created, based on the aggregated ratings of personality disorder experts. These prototypes agree well with DSM diagnostic criteria. [20] The Five-Factor prototypes also reflected the high comorbidity rates of personality disorders. This is explained by the idea that various other disorders tap into dimensions that overlap with those of the primary diagnosis. [20]
Another Five-Factor based technique involves diagnosing personality disorders based on clinician ratings of various facets of the five factors (e.g. self-consciousness, which falls under the neuroticism factor; excitement seeking, which falls under the extraversion factor). This technique is partially based on the prototype model, as each facet's "score" is based on its rating of how prototypical it is of each personality disorder, with prototypically low facets (with a score less than 2) reverse-scored. Using this technique, diagnosis is based on an individual's summed score across relevant facets. This summed-score technique has been shown to be as sensitive as the prototype technique, and the easier computation method makes it a useful suggested screening technique. [6]
The Five-Factor assessment of personality disorders has also been correlated with the Psychopathy Resemblance Index of the NEO Personality Inventory, as well as with the individual personality dimensions of the NEO-PI-R. [21] It also resolves several issues regarding the PCL-R psychopathy assessment, as a Five-Factor-based re-interpretation of the PCL-R factor structure shows that the “Aggressive Narcissism” factor taps into facets of low agreeableness (with some contribution of facets of neuroticism and extraversion), and the “Socially deviant lifestyle” factor represents facets of low conscientiousness and low agreeableness. It has also been shown that the sex differences in personality disorders can be reasonably predicted by sex differences in Big 5 traits. [22]
Criticism
The dimension of openness to experience of the Five-Factor model has been criticized for not directly relating to any of the major characteristics of personality disorders in the same way as do the other four dimensions [ citation needed ]. It has been suggested that schizotypal and histrionic personality disorders could be partially characterized by high levels of openness to experience (in the forms of openness to ideas and feelings, respectively) [ citation needed ], while obsessive-compulsive, paranoid, schizoid, and avoidant personality disorders can all be conceptualized by extremely low levels of openness [ citation needed ]. However, there is little to no empirical support for this hypothesis, particularly with schizotypal personality disorder. Additionally, the Openness scale of the NEO-PI-R, which is one of the most widely used measures of Big Five traits, was based on research and theory which viewed openness (such as self-actualization and personal growth) as beneficial, so measurement of extreme openness using the NEO-PI-R, is actually a marker of good mental health. [5]
Seven factor model
The Five-Factor approach has been criticized for being limited in some respects in its conceptualization of personality disorders. This limitation is due to the fact that it does not include evaluative trait terms such as “bad”, “awful”, or “vicious”. Some research has suggested that two evaluative dimensions should be added to the Five-Factor model of personality disorders. Empirical support for this approach comes from factor analyses that include the Big Five factors and evaluative terms. These analyses show that the evaluative terms contribute to two additional factors, one each for positive and negative valence. The addition of these two factors resolves much of the ambiguity of the openness dimension in the Five-Factor approach, as the openness factor changes to a conventionality factor, and adjectives such as “odd”, “strange”, and “weird” (which all characterize schizotypal personality disorder) fall onto the negative valence factor. These results indicate that the inclusion of evaluative terms and valence dimensions can be valuable for better describing the extreme and maladaptive levels of personality traits that comprise personality disorder profiles. [5]
Internalizing/Externalizing model
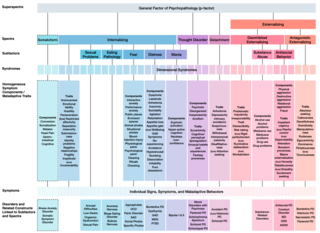
A two-factor model of psychopathology in general has also been suggested, in which most disorders fall along internalizing and externalizing dimensions, [23] [24] which encompass mood and anxiety disorders, and antisocial personality and substance use disorders, respectively. [24] Although this approach was originally developed to understand psychopathology in general, it has often been focused to apply to personality disorders, such as borderline personality disorder to help better understand patterns of comorbidity. [25]
Szondi drive theory
Hungarian psychiatrist Léopold Szondi formulated in 1935 a dimensional model of personality comprising four dimensions and eight drives ("facets" in DSM V terminology). It was based on a drive theory, in which the four dimensions correspond to the independent hereditary circular mental diseases established by the psychiatric genetics of the time: [26] the schizoform (containing the paranoid and the catatonic drives), the manic-depressive (for the "contact" dimension), the paroxysmal (including the epileptic and hysteric drives), and the sexual drive disorder (including the hermaphrodite and the sadomasochist drives). [27] The Sex (S) and Contact (C) dimensions can be further grouped as representing pulsions at the border with the outer world, while the Paroximal (P) and Schizoform (Sch) dimensions at the inner part of the psyche.
Integrated models
Network analysis
Network analysis diverts most strongly from the categorical approach because it assumes that the symptoms of a disorder have a causal relationship to each other. This theoretical assumption is made because no mental disorder can currently be understood as existing independently from its symptoms, as other medical diseases can be. According to the network approach symptoms are not looked at as the product of a set of latent disorders, instead they are looked at as mutually interacting and reciprocally reinforcing elements within a wider network. [28] Therefore, a diagnosis is not needed to understand why the symptoms hang together. Clusters of densely connected symptoms can be defined as disorders, but they are inevitably intertwined with related symptoms and cannot be entirely separated. This helps explain the growing body of research showing comorbidity, co-occurring genetic markers and co-occurring symptoms across personality disorders. [29]
Therapeutic consequences
The therapeutic consequence of this is that treatment is targeted at the symptoms themselves and the causal relations between them, not the overarching diagnosis. This is because targeting the diagnosis is trying to treat an unspecified summary of a complex collection of causes. Adopting this attitude sits well with the therapeutic treatments in use at the moment that have the strongest evidence base. [29]
Network construction
Network analysis has its roots in mathematics and physics but is increasingly being used in other areas. Essentially it is a method of analyzing mutually interacting entities by represented them as nodes which are connected to through relations called edges. Edges represent any sort of relation such as a partial correlation. Complex network analyses of other subjects have looked at tipping points, where one system suddenly transitions into another, such as when a tropical forests goes into a savannah. If these could be identified in individual's psychopathological dynamic networks then they could be used to determine when a person's network is on the brink of collapse and what can be done to alter it. [29]
Criticisms
There are concerns that the network modal does not have enough parsimony and is too difficult to interpret. [30]