Signs and symptoms
Socially, psychopathy typically involves extensive callous and manipulative self-serving behaviors with no regard for others and often is associated with repeated delinquency, crime, and violence. Mentally, impairments in processes related to affect and cognition, particularly social mental processes, have also been found. Developmentally, symptoms of psychopathy have been identified in young children with conduct disorder and suggest at least a partial constitutional factor that influences its development. [21]
Primary features
There is disagreement over which features should be considered part of psychopathy, with researchers identifying around 40 traits supposedly indicative of the construct, [22] [23] though the following characteristics are almost universally considered central.
Core traits
In 2001, David J. Cooke and Christine Michie [24] proposed a three-factor model of the Psychopathy Checklist-Revised, which has seen widespread application in other measures, such as the Youth Psychopathic Traits Inventory [25] and Antisocial Process Screening Device. [26]
- Arrogant and deceitful interpersonal style: impression management or superficial charm, inflated and grandiose sense of self-worth, pathological lying/deceit, and manipulation for personal gain.
- Deficient affective experience: lack of remorse or guilt, shallow affect (coldness and unemotionality), callousness and lack of empathy, and failure to accept responsibility for one's own actions.
- Impulsive and irresponsible lifestyle: impulsivity, sensation-seeking and risk-taking, irresponsible and unreliable behavior, financially parasitic lifestyle, and a lack of realistic, long-term goals.
Low anxiety and fearlessness
Hervey M. Cleckley's 1941 original description of psychopathy included the absence of nervousness and neurotic disorders, and later theorists referred to psychopaths as fearless or thick-skinned. [27] While it is often claimed that the Psychopathy Checklist-Revised (PCL-R) does not include low anxiety or fearlessness, such features do contribute to the scoring of the Facet 1 (interpersonal) items, mainly through self-assurance, unrealistic optimism, brazenness, and imperturbability. [28] Indeed, while self-report studies have been inconsistent using the two-factor model of the PCL-R, studies which separate Factor 1 into interpersonal and affective facets, more regularly show modest associations between Facet 1 and low anxiety, boldness and fearless dominance (especially items assessing glibness/charm and grandiosity). [29] [30] [31] When both psychopathy and low anxiety/boldness are measured using interviews, both interpersonal and affective facets are both associated with fearlessness and lack of internalizing disorders. [32] [33] [34]
The importance of low anxiety/fearlessness to psychopathy has historically been underscored through behavioral and physiological studies showing diminished responses to threatening stimuli (interpersonal and affective facets both contributing). [35] However, it is not known whether this is reflected in the reduced experience of state fear or where it reflects impaired detection and response to threat-related stimuli. [36] Moreover, such deficits in threat responding are known to be reduced or even abolished when attention is focused on the threatening stimuli.
Offending
Criminality

In terms of simple correlations, the PCL-R manual states that an average score of 22.1 has been found in North American prisoner samples, and that 20.5% scored 30 or higher. An analysis of prisoner samples from outside North America found a somewhat lower average value of 17.5. Studies have found that psychopathy scores correlated with repeated imprisonment, detention in higher security, disciplinary infractions, and substance misuse. [37] [38]
Psychopathy, as measured with the PCL-R in institutional settings, shows in meta-analyses small to moderate effect sizes with institutional misbehavior, post-release crime, or post-release violent crime, with similar effects for the three outcomes. Individual studies give similar results for adult offenders, forensic psychiatric samples, community samples, and youth. The PCL-R is poorer at predicting sexual re-offending. This small to moderate effect appears to be largely due to the scale items assessing impulsive behaviors and past criminal history, which are well-established but very general risk factors. The aspects of core personality often held to be distinctively psychopathic generally show little or no predictive link to crime by themselves. For example, Factor 1 of the PCL-R and Fearless Dominance of the PPI-R have a smaller or no relationship to crime, including violent crime. In contrast, Factor 2 and Impulsive antisociality of the PPI-R are associated more strongly with criminality. Factor 2 has a relationship of similar strength to that of the PCL-R as a whole. The antisocial facet of the PCL-R is still predictive of future violence after controlling for past criminal behavior, which, together with results regarding the PPI-R, which by design does not include past criminal behavior, suggests that impulsive behaviors are an independent risk factor. Thus, the concept of psychopathy may perform poorly when attempted to be used as a general theory of crime. [12] [39]
Violence
Studies have suggested a strong correlation between psychopathy scores and violence, and the PCL-R emphasizes features that are somewhat predictive of violent behavior. Researchers, however, have noted that psychopathy is dissociable from and not synonymous with violence. [12] [40]
It has been suggested that psychopathy is associated with "instrumental aggression", also known as predatory, proactive, or "cold-blooded" aggression, a form of aggression characterized by reduced emotion and conducted with a goal differing from but facilitated by the commission of harm. [41] [42] One conclusion in this regard was made by a 2002 study of homicide offenders, which reported that the homicides committed by homicidal offenders with psychopathy were almost always (93.3%) primarily instrumental, significantly more than the proportion (48.4%) of those committed by non-psychopathic homicidal offenders, with the instrumentality of the homicide also correlated with the total PCL-R score of the offender as well as their scores on the Factor 1 "interpersonal-affective" dimension. However, contrary to the equating of this to mean exclusively "in cold blood", more than a third of the homicides committed by psychopathic offenders involved some component of emotional reactivity as well. [43] In any case, FBI profilers indicate that serious victim injury is generally an emotional offense, and some research supports this, at least concerning sexual offending. One study has found more serious offending by non-psychopathic offenders on average than by offenders with psychopathy (e.g., more homicides versus more armed robbery and property offenses), and another has found that the Affective facet of the PCL-R predicted reduced offense seriousness. [12]
Studies on perpetrators of domestic violence find that abusers have high rates of psychopathy, with the prevalence estimated to be at around 15-30%. Furthermore, the commission of domestic violence is correlated with Factor 1 of the PCL-R, which describes the emotional deficits and the callous and exploitative interpersonal style found in psychopathy. The prevalence of psychopathy among domestic abusers indicate that the core characteristics of psychopathy, such as callousness, remorselessness, and a lack of close interpersonal bonds, predispose those with psychopathy to committing domestic abuse, and suggest that the domestic abuses committed by these individuals are callously perpetrated (i.e. instrumentally aggressive) rather than a case of emotional aggression and therefore may not be amenable to the types of psychosocial interventions commonly given to domestic abuse perpetrators. [42] [44]
Some clinicians suggest that assessment of the construct of psychopathy does not necessarily add value to violence risk assessment. A large systematic review and meta-regression found that the PCL performed the poorest out of nine tools for predicting violence. In addition, studies conducted by the authors or translators of violence prediction measures, including the PCL, show, on average, more positive results than those conducted by more independent investigators. Several other risk assessment instruments can predict future crime with an accuracy similar to that of the PCL-R, and some are considerably easier, quicker, and less expensive to administer. This may even be done automatically by a computer, based on data such as age, gender, number of prior convictions, and age at first conviction. Some of these assessments may also identify treatment changes and goals, identify quick changes that may help short-term management, identify more specific kinds of violence that may be at risk, and establish specific probabilities of offending for specific scores. Nonetheless, the PCL-R may remain popular for risk assessment due to its pioneering role and extensive research using it. [12] [45] [46] [47] [48] [49] [50]
The U.S. Federal Bureau of Investigation (FBI) reports that psychopathic behavior is consistent with traits common to some serial killers, including sensation seeking, a lack of remorse or guilt, impulsivity, the need for control, and predatory behavior. [51] It has also been found that the homicide victims of psychopathic offenders were disproportionately female in comparison to the more equitable gender distribution of victims of non-psychopathic offenders. [43]
Sexual offending
Psychopathy has been associated with the commission of sexual crime, with some researchers arguing that it is correlated with a preference for violent sexual behavior. A 2011 study of conditional releases for Canadian male federal offenders found that psychopathy was related to more violent and non-violent offences, but not more sexual offences. [52] For child molesters, psychopathy was associated with more offences. [53] A study on the relationship between psychopathy scores and types of aggression in a sample of sexual murderers, in which 84.2% of the sample had PCL-R scores above 20 and 47.4% above 30, found that 82.4% of those with scores above 30 had engaged in sadistic violence (defined as enjoyment indicated by self-report or evidence) compared to 52.6% of those with scores below 30, and total PCL-R and Factor 1 scores correlated significantly with sadistic violence. [54] [55] Despite this, it is reported that offenders with psychopathy (both sexual and non-sexual offenders) are about 2.5 times more likely to be granted conditional release compared to non-psychopathic offenders. [53]
Hildebrand and colleagues (2004) have uncovered an interaction between psychopathy and deviant sexual interests, wherein those high in psychopathy who also endorsed deviant sexual interests were more likely to recidivate sexually. [56] A subsequent meta-analysis has consolidated such a result. [57]
In considering the issue of possible reunification of some sex offenders into homes with a non-offending parent and children, it has been advised that any sex offender with a significant criminal history should be assessed on the PCL-R, and if they score 18 or higher, then they should be excluded from any consideration of being placed in a home with children under any circumstances. [58] There is, however, increasing concern that PCL scores are too inconsistent between different examiners, including in its use to evaluate sex offenders. [59]
Other offending
The possibility of psychopathy has been associated with organized crime, economic crime, and war crimes. Terrorists are sometimes considered psychopathic, and comparisons may be drawn with traits such as antisocial violence, a selfish worldview that precludes the welfare of others, a lack of remorse or guilt, and blame externalization. [60] However, John Horgan, author of The Psychology of Terrorism, argues that such comparisons could also then be drawn more widely: for example, to soldiers in wars. Coordinated terrorist activity requires organization, loyalty, and ideological fanaticism often to the extreme of sacrificing oneself for an ideological cause. Traits such as a self-centered disposition, unreliability, poor behavioral controls, and unusual behaviors may disadvantage or preclude psychopathic individuals from conducting organized terrorism. [61] [62]
It may be that a significant portion of people with psychopathy are socially successful and tend to express their antisocial behavior through more covert avenues, such as social manipulation or white collar crime. Such individuals are sometimes referred to as "successful psychopaths" and may not necessarily always have extensive histories of traditional antisocial behavior as characteristic of traditional psychopathy. [63]
Childhood and adolescent precursors
The PCL:YV is an adaptation of the PCL-R for individuals aged 13–18 years. It is, like the PCL-R, done by a trained rater based on an interview and an examination of criminal and other records. The "Antisocial Process Screening Device" (APSD) is also an adaptation of the PCL-R. It can be administered by parents or teachers for individuals aged 6–13 years. High psychopathy scores for both juveniles (as measured with these instruments) and adults (as measured with the PCL-R and other measurement tools) have similar associations with other variables, including similar ability in predicting violence and criminality. [12] [64] [65] Juvenile psychopathy may also be associated with more negative emotionality such as anger, hostility, anxiety, and depression. [12] [66] Psychopathic traits in youth typically comprise three factors: callous/unemotional, narcissism, and impulsivity/irresponsibility. [67] [68]
There is a positive correlation between early negative life events of the ages 0–4 and the emotion-based aspects of psychopathy. [69] There are moderate to high correlations between psychopathy rankings from late childhood to early adolescence. The correlations are considerably lower from early- or mid-adolescence to adulthood. In one study, most of the similarities were on the Impulsive- and Antisocial-Behavior scales. Of those adolescents who scored in the top 5% highest psychopathy scores at age 13, less than one-third (29%) were classified as psychopathic at age 24. Some recent studies have also found a poorer ability to predict long-term, adult offending. [12] [70]
Conduct disorder
Conduct disorder is diagnosed based on a prolonged pattern of antisocial behavior in childhood or adolescence, and may be seen as a precursor to ASPD. Some researchers have speculated that two subtypes of conduct disorder mark dual developmental pathways to adult psychopathy. [12] [71] [72] The DSM allows differentiating between childhood onset before age 10 and adolescent onset at age 10 and later. Childhood-onset is argued to be more due to a personality disorder caused by neurological deficits interacting with an adverse environment. For many, but not all, childhood onset is associated with what Terrie Moffitt's developmental theory of crime refers to as "life-course-persistent" antisocial behavior as well as poorer health and economic status. Adolescent onset is argued to more typically be associated with short-term antisocial behavior. [12]
It has been suggested that the combination of early-onset conduct disorder and ADHD may be associated with life-course-persistent antisocial behaviors as well as psychopathy. There is evidence that this combination is more aggressive and antisocial than those with conduct disorder alone. However, it is not a particularly distinct group since the vast majority of young children with conduct disorder also have ADHD. Some evidence indicates that this group has deficits in behavioral inhibition, similar to those of adults with psychopathy. They may not be more likely than those with conduct disorder alone to have the interpersonal/affective features and the deficits in emotional processing characteristic of adults with psychopathy. Proponents of different types/dimensions of psychopathy have seen this type as possibly corresponding to adult secondary psychopathy and increased disinhibition in the triarchic model. [12]
The DSM-5 includes a specifier for those with conduct disorder who also display a callous, unemotional interpersonal style across multiple settings and relationships. [69] The specifier is based on research that suggests that those with conduct disorder who also meet the criteria for the specifier tend to have a more severe form of the disorder with an earlier onset, as well as a different response to treatment. Proponents of different types/dimensions of psychopathy have seen this as possibly corresponding to adult primary psychopathy and increased boldness or meanness in the triarchic model. [12] [73]
Mental traits
Cognition
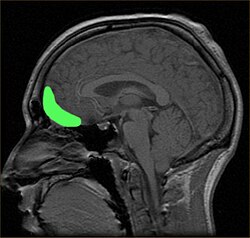
Dysfunctions in the prefrontal cortex and amygdala regions of the brain have been associated with specific learning impairments in psychopathy. Damage to the ventromedial prefrontal cortex, which regulates the activity in the amygdala, leads to common characteristics in psychopathic individuals. [74] Since the 1980s, scientists have linked traumatic brain injury, including damage to these regions, with violent and psychopathic behavior. Patients with damage in such areas resembled "psychopathic individuals" whose brains were incapable of acquiring social and moral knowledge; those who acquired damage as children may have trouble conceptualizing social or moral reasoning, while those with adult-acquired damage may be aware of proper social and moral conduct but be unable to behave appropriately. Dysfunctions in the amygdala and ventromedial prefrontal cortex may also impair stimulus-reinforced learning in psychopaths, whether punishment-based or reward-based. People scoring 25 or higher in the PCL-R, with an associated history of violent behavior, appear to have significantly reduced mean microstructural integrity in their uncinate fasciculus—white matter connecting the amygdala and orbitofrontal cortex. There is evidence from DT-MRI of disruptions in white-matter connections between these two important areas. [75] [76] [77]
Although some studies have suggested inverse relationships between psychopathy and intelligence, including with regards to verbal IQ, Hare and Neumann state that a large literature demonstrates at most only a weak association between psychopathy and IQ, noting that the early pioneer Cleckley included good intelligence in his checklist due to selection bias (since many of his patients were "well educated and from middle-class or upper-class backgrounds") and that "there is no obvious theoretical reason why the disorder described by Cleckley or other clinicians should be related to intelligence; some psychopaths are bright, others less so". Studies also indicate that different aspects of the definition of psychopathy (e.g., interpersonal, affective (emotion), behavioral, and lifestyle components) can show different links to intelligence, and the result can depend on the type of intelligence assessment (e.g., verbal, creative, practical, analytical). [19] [40] [78] [79]
Emotion recognition and empathy
A large body of research suggests that psychopathy is associated with atypical responses to distress cues from other people, more precisely an impaired emotional empathy in the recognition of, and response to, facial expressions, body gestures and vocal tones of fear, sadness, pain and happiness. [80] [21] This impaired recognition and reduced autonomic responsiveness might be partly accounted for by a decreased activation of the fusiform and extrastriate cortical regions. [21] The underlying biological surfaces for processing expressions of happiness are functionally intact in psychopaths, although less responsive than those of controls. The neuroimaging literature is unclear about whether deficits are specific to particular emotions, such as fear. The overall pattern of results across studies indicates that people diagnosed with psychopathy demonstrate reduced MRI, fMRI, aMRI, PET, and SPECT activity in areas of the brain. [81] Research has also shown that an approximate 18% smaller amygdala size contributes to a significantly lower emotional sensation in regards to fear, sadness, amongst other negative emotions, which may likely be the reason as to why psychopathic individuals have lower empathy. [82] Some recent fMRI studies have reported that emotion perception deficits in psychopathy are pervasive across emotions (positives and negatives). [83] [84] [85] [86] [87] Studies on children with psychopathic tendencies have also shown such associations. [87] [88] [89] [90] [91] [92] Meta-analyses have also found evidence of impairments in both vocal and facial emotional recognition for several emotions (i.e., not only fear and sadness) in both adults and children/adolescents. [92]
Moral judgment
Psychopathy has been associated with amorality—an absence of, indifference towards, or disregard for moral beliefs. There is little firm data on patterns of moral judgment. Studies of the developmental level (sophistication) of moral reasoning found all possible results—lower, higher, or the same as non-psychopaths. Studies that compared judgments of personal moral transgressions versus judgments of breaking conventional rules or laws found that psychopaths rated them as equally severe, whereas non-psychopaths rated the rule-breaking as less severe. [93]
A study comparing judgments of whether personal or impersonal harm would be endorsed to achieve the rational maximum (utilitarian) amount of welfare found no significant differences between subjects high and low in psychopathy. However, a further study using the same tests found that prisoners scoring high on the PCL were more likely to endorse impersonal harm or rule violations than non-psychopathic controls were. The psychopathic offenders who scored low in anxiety were also more willing to endorse personal harm on average. [93]
Assessing accidents, where one person harmed another unintentionally, psychopaths judged such actions to be more morally permissible. This result has been considered a reflection of psychopaths' failure to appreciate the emotional aspect of the victim's harmful experience. [94]