| McBurney's point | |
|---|---|
 Location of McBurney's point (1), located two thirds the distance from the umbilicus (2) to the right anterior superior iliac spine (3) | |
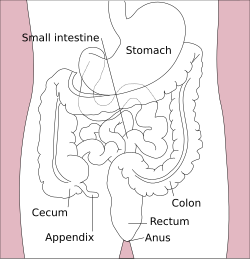
 Surface projections of the organs of the trunk, with McBurney's point labeled with a red circle at bottom left at the inferior part of the cecum | |
| Identifiers | |
| FMA | 11362 |
| Anatomical terminology | |
McBurney's point is the point over the right side of the abdomen that is one-third of the distance from the anterior superior iliac spine to the umbilicus (navel). This is near the most common location of the appendix.