Depending on a patient's condition, their toileting needs may need to be met differently. This could be by assisting the patient to walk to a toilet, to a bedside commode chair, onto a bedpan, or to provide a male patient with a urinal. A more dependent or incontinent patient may have their toileting needs met solely through the use of adult diapers. Other options are incontinence pads and urinary catheters.
Ambulatory assistance
Some patients can walk with assistance from another person, usually a health care worker. Aside from the need for this help, they are capable of meeting their own elimination needs.
Bedpan
Patients who cannot get out of bed easily but who can control their bladder and bowels are able to request a bedpan. The bedpan is placed underneath the patient, who can urinate or defecate as needed.
Some patients are able to place their own bedpans under themselves, and assistance is required only to empty them after the fact.
Urinal
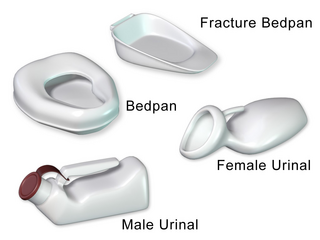
A urinal is much like a bedpan but only for a male, the urinal is shaped in a way that the male may use it while still in bed and remain comfortable. The urinal is also often used when input and output (I & O) must be recorded.
Briefs
Incontinent patients often wear briefs to prevent their trousers from being stained by their elimination. Briefs must be checked and changed frequently.
Catheter
Catheters, in this sense, are tubes that drain urine from the body. A Foley catheter, used with men and women, is inserted into the bladder. An external catheter is attached to the penis of a male patient. In the US, while Foley catheters can only be applied by a nurse or physician, external catheters can be attached by a certified nurse assistant.
Collection, measurement, and analysis
Input and output
Input and output (I & O) is the measure of food and fluids that enter and exit the body. Certain patients with the need are placed on I & O, and if so, their urinary output is measured.
With self-toileting patients on I & O, or those who are assisted to a regular toilet or portable commode, a receptacle is placed in the toilet bowl that catches all urine that is put out by the patient. This, in turn, is measured by the nursing staff and recorded prior to its disposal.
If the patient is using a bedpan, the nursing staff member who empties the bedpan measures the urine prior to its disposal.
Urinals usually contain measuring lines providing easy measurement. Urinals are also useful for measuring urine from other sources.
Catheters, which are frequently used when it is necessary to measure a patient's output, often have measuring lines on their bags, but these are not considered to be accurate because the bag is floppy. Urine that is emptied from a catheter must be placed in a level container (such as a urinal) in order to be measured.
Bowel movement
In many patients, bowel movement is also measured. In some facilities, it is the standard procedure to record bowel movement of all patients.
Bowel movement is generally measured by its size (small, medium, or large), given the amount. Additionally, if a patient has diarrhea, this is recorded.
A patient who has not had a bowel movement in several days is often given laxatives. Patients who independently toilet themselves often do not report bowel movements, thereby leading them to get laxatives when they do not need them.[citation needed]
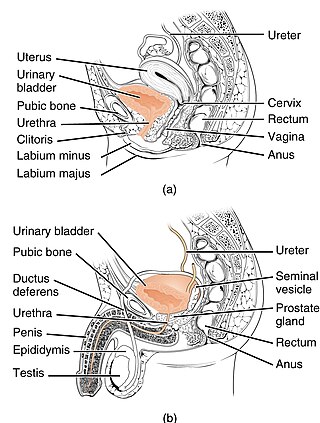
Urination is the release of urine from the bladder to the outside of the body. Urine is released from the urethra through the penis or vulva in placental mammals and through the cloaca in other vertebrates. It is the urinary system's form of excretion. It is also known medically as micturition, voiding, uresis, or, rarely, emiction, and known colloquially by various names including peeing, weeing, pissing, and euphemistically going number one. The process of urination is under voluntary control in healthy humans and other animals, but may occur as a reflex in infants, some elderly individuals, and those with neurological injury. It is normal for adult humans to urinate up to seven times during the day.
Urinary incontinence (UI), also known as involuntary urination, is any uncontrolled leakage of urine. It is a common and distressing problem, which may have a large impact on quality of life. It has been identified as an important issue in geriatric health care. The term enuresis is often used to refer to urinary incontinence primarily in children, such as nocturnal enuresis. UI is an example of a stigmatized medical condition, which creates barriers to successful management and makes the problem worse. People may be too embarrassed to seek medical help, and attempt to self-manage the symptom in secrecy from others.
In urinary catheterization, a latex, polyurethane, or silicone tube known as a urinary catheter is inserted into the bladder through the urethra to allow urine to drain from the bladder for collection. It may also be used to inject liquids used for treatment or diagnosis of bladder conditions. A clinician, often a nurse, usually performs the procedure, but self-catheterization is also possible. A catheter may be in place for long periods of time or removed after each use.
Urinary retention is an inability to completely empty the bladder. Onset can be sudden or gradual. When of sudden onset, symptoms include an inability to urinate and lower abdominal pain. When of gradual onset, symptoms may include loss of bladder control, mild lower abdominal pain, and a weak urine stream. Those with long-term problems are at risk of urinary tract infections.
In urology, a Foley catheter is one of many types of urinary catheters (UC). The Foley UC was named after Frederic Foley, who produced the original design in 1929. Foleys are indwelling UC, often referred to as an IDCs. This differs from in/out catheters. The UC is a flexible tube if it is indwelling and stays put, or rigid if it is in/out, that a clinician, or the client themselves, often in the case of in/out UC, passes it through the urethra and into the bladder to drain urine.
A bedpan or bed pan is a device used as a receptacle for the urine and/or feces of a person who is confined to a bed and therefore not able to use a toilet or chamber pot.
The Mitrofanoff procedure, also known as the Mitrofanoff appendicovesicostomy, is a surgical procedure in which the appendix is used to create a conduit, or channel, between the skin surface and the urinary bladder. The small opening on the skin surface, or the stoma, is typically located either in the navel or nearby the navel on the right lower side of the abdomen. Originally developed by Professor Paul Mitrofanoff in 1980, the procedure represents an alternative to urethral catheterization and is sometimes used by people with urethral damage or by those with severe autonomic dysreflexia. An intermittent catheter, or a catheter that is inserted and then removed after use, is typically passed through the channel every 3–4 hours and the urine is drained into a toilet or a bottle. As the bladder fills, rising pressure compresses the channel against the bladder wall, creating a one-way valve that prevents leakage of urine between catheterizations.
A suprapubic cystostomy or suprapubic catheter (SPC) is a surgically created connection between the urinary bladder and the skin used to drain urine from the bladder in individuals with obstruction of normal urinary flow. The connection does not go through the abdominal cavity.
A ureteral stent, or ureteric stent, is a thin tube inserted into the ureter to prevent or treat obstruction of the urine flow from the kidney. The length of the stents used in adult patients varies between 24 and 30 cm. Additionally, stents come in differing diameters or gauges, to fit different size ureters. The stent is usually inserted with the aid of a cystoscope. One or both ends of the stent may be coiled to prevent it from moving out of place; this is called a JJ stent, double J stent or pig-tail stent.
A urine collection device or UCD is a device that allows the collection of urine for analysis or for purposes of simple elimination. UCDs of the latter type are sometimes called piddle packs.
Neurogenic bladder dysfunction, often called by the shortened term neurogenic bladder, refers to urinary bladder problems due to disease or injury of the central nervous system or peripheral nerves involved in the control of urination. There are multiple types of neurogenic bladder depending on the underlying cause and the symptoms. Symptoms include overactive bladder, urinary urgency, frequency, incontinence or difficulty passing urine. A range of diseases or conditions can cause neurogenic bladder including spinal cord injury, multiple sclerosis, stroke, brain injury, spina bifida, peripheral nerve damage, Parkinson's disease, multiple system atrophy or other neurodegenerative diseases. Neurogenic bladder can be diagnosed through a history and physical as well as imaging and more specialized testing. In addition to symptomatic treatment, treatment depends on the nature of the underlying disease and can be managed with behavioral changes, medications, surgeries, or other procedures. The symptoms of neurogenic bladder, especially incontinence, can severely degrade a person's quality of life.
A ureterostomy is the creation of a stoma for a ureter or kidney.
A prostatic stent is a stent used to keep open the male urethra and allow the passing of urine in cases of prostatic obstruction and lower urinary tract symptoms (LUTS). Prostatic obstruction is a common condition with a variety of causes. Benign prostatic hyperplasia (BPH) is the most common cause, but obstruction may also occur acutely after treatment for BPH such as transurethral needle ablation of the prostate (TUNA), transurethral resection of the prostate (TURP), transurethral microwave thermotherapy (TUMT), prostate cancer or after radiation therapy.
Cystometry, also known as flow cystometry, is a clinical diagnostic procedure used to evaluate bladder function. Specifically, it measures contractile force of the bladder when voiding. The resulting chart generated from cystometric analysis is known as a cystometrogram (CMG), which plots intravesical pressure against the volume of fluid in the bladder.
A urinal, urine bottle, or male urinal is a bottle for urination. It is most frequently used in health care for patients who find it impossible or difficult to get out of bed during sleep. Urinals allow the patient who has cognition and movement of their arms to urinate without the help of staff. A urinal bottle can also be used by travelers or transportation workers who are unable to immediately use a public restroom as part of an emergency kit, or in areas where restroom facilities are too distant.
Urodynamic testing or urodynamics is a study that assesses how the bladder and urethra are performing their job of storing and releasing urine. Urodynamic tests can help explain symptoms such as:
Overflow incontinence is a concept of urinary incontinence, characterized by the involuntary release of urine from an overfull urinary bladder, often in the absence of any urge to urinate. This condition occurs in people who have a blockage of the bladder outlet, or when the muscle that expels urine from the bladder is too weak to empty the bladder normally. Overflow incontinence may also be a side effect of certain medications.
Intermittent catheterization is a medical technique used in conditions where patients need either short-term catheter-based management of the urinary bladder or as a daily habit for life. Intermittent catheterization is considered the "gold standard" for medical bladder emptying. Intermittent catheterization can be done by the patient or a caregiver in a home environment.
In biology, Inputand output (I&O) is the measure of food and fluids that enter and exit the body. Certain patients with the need are placed on I & O, and if so, their urinary output is measured.
Suprapubic aspiration is a procedure to take a urine sample. It involves putting a needle through the skin just above the pubic bone into the bladder. It is typically used as a method to collect urine in child less than 2 years of age who is not yet toilet trained in an effort to diagnose a urinary tract infection.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.