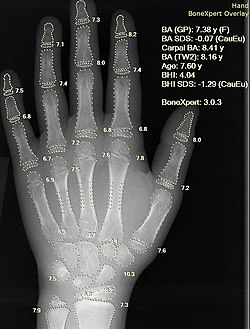
X-ray of a hand, with automatic calculation of bone age by a computer software
Artificial intelligence in healthcare is the application of artificial intelligence (AI) to analyze and understand complex medical and healthcare data. In some cases, it can exceed or augment human capabilities by providing better or faster ways to diagnose, treat, or prevent disease.[1][2][3][4]
Using AI in healthcare presents unprecedented ethical concerns related to issues such as data privacy, automation of jobs, and amplifying already existing algorithmic bias.[11] New technologies such as AI are often met with resistance by healthcare leaders, leading to slow and erratic adoption.[12] There have been cases where AI has been put to use in healthcare without proper testing.[13][14][15][16] A systematic review and thematic analysis in 2023 showed that most stakeholders including health professionals, patients, and the general public doubted that care involving AI could be empathetic.[17] Meta-studies have found that the scientific literature on AI in healthcare often suffers from a lack of reproducibility.[18][19][20][21]
Applications in healthcare systems
Disease diagnosis
Accurate and early diagnosis of diseases is still a challenge in healthcare. Recognizing medical conditions and their symptoms is a complex problem. AI can assist clinicians with data processing capabilities to save time and improve accuracy.[22] Through the use of machine learning, artificial intelligence can substantially aid doctors in patient diagnosis through the analysis of mass electronic health records (EHRs).[23] AI can help early prediction, for example, of Alzheimer's disease and dementias, by looking through large numbers of similar cases and possible treatments.[24]
In 2023 a study reported higher satisfaction rates with ChatGPT-generated responses compared with those from physicians for medical questions posted on Reddit's r/AskDocs.[25] Evaluators preferred ChatGPT's responses to physician responses in 78.6% of 585 evaluations, noting better quality and empathy. The authors noted that these were isolated questions taken from an online forum, not in the context of an established patient-physician relationship.[25] Moreover, responses were not graded on the accuracy of medical information, and some have argued that the experiment was not properly blinded, with the evaluators being coauthors of the study.[26][27][28]
A 2025 meta-analysis in PLOS One found that the use of AI algorithms for detecting tooth decay was clinically justified.[30]
Electronic health records
Electronic health records (EHR) are crucial to the digitalization and information spread of the healthcare industry. Now that around 80% of medical practices use EHR, some anticipate the use of artificial intelligence to interpret the records and provide new information to physicians.[31]
One application uses natural language processing (NLP) to make more succinct reports that limit the variation between medical terms by matching similar medical terms.[31] For example, the term heart attack and myocardial infarction mean the same things, but physicians may use one over the other based on personal preferences.[31] NLP algorithms consolidate these differences so that larger datasets can be analyzed.[31] Another use of NLP identifies phrases that are redundant due to repetition in a physician's notes and keeps the relevant information to make it easier to read.[31] Other applications use concept processing to analyze the information entered by the current patient's doctor to present similar cases and help the physician remember to include all relevant details.[32]
Beyond making content edits to an EHR, there are AI algorithms that evaluate an individual patient's record and predict a risk for a disease based on their previous information and family history.[33] One general algorithm is a rule-based system that makes decisions similarly to how humans use flow charts.[34] This system takes in large amounts of data and creates a set of rules that connect specific observations to concluded diagnoses.[34] Thus, the algorithm can take in a new patient's data and try to predict the likelihood that they will have a certain condition or disease.[34] Since the algorithms can evaluate a patient's information based on collective data, they can find any outstanding issues to bring to a physician's attention and save time.[33] One study conducted by the Centerstone research institute found that predictive modeling of EHR data has achieved 70–72% accuracy in predicting individualized treatment response.[35] These methods are helpful due to the fact that the amount of online health records doubles every five years.[33] Physicians do not have the bandwidth to process all this data manually, and AI can leverage this data to assist physicians in treating their patients.[33]
Clinical documentation
The use of generative artificial intelligence (GenAI) tools (a subset of AI) is growing as a support for clinical documentation, primarily for transcribing consultations and drafting medical notes. Early studies have shown that such tools, may assist clinicians with documentation tasks, reducing administrative burdens, which are known drivers of burnout [36][37][38]. These tools may also improve accessibility for patients [39][40] synthesizing complex data, and writing responses in a desired conversational style or literacy level [41][42] ultimately improving the overall efficiency of healthcare services [43][44]
AlphaFold and drug discovery
AlphaFold has the ability to predict protein structures based on the constituent amino acid sequence, expected to have benefits in the life sciences--accelerating drug discovery and enabling better understanding of diseases.[45] Nobel laureate Venki Ramakrishnan called the result "a stunning advance on the protein folding problem", adding that "It has occurred decades before many people in the field would have predicted. It will be exciting to see the many ways in which it will fundamentally change biological research." In 2023, Demis Hassabis and John Jumper won the Breakthrough Prize in Life Sciences[46] as well as the Albert Lasker Award for Basic Medical Research for their management of the AlphaFold project.[47] Hassabis and Jumper proceeded to win the Nobel Prize in Chemistry in 2024 for their work on "protein structure prediction" with David Baker of the University of Washington.[48][49]
Drug interactions
Improvements in natural language processing led to the development of algorithms to identify drug-drug interactions in medical literature.[50][51][52][53] Drug-drug interactions pose a threat to those taking multiple medications simultaneously, and the danger increases with the number of medications being taken.[54] To address the difficulty of tracking all known or suspected drug-drug interactions, machine learning algorithms have been created to extract information on interacting drugs and their possible effects from medical literature. Efforts were consolidated in 2013 in the DDIExtraction Challenge, in which a team of researchers at Carlos III University assembled a corpus of literature on drug-drug interactions to form a standardized test for such algorithms.[55] Competitors were tested on their ability to accurately determine, from the text, which drugs were shown to interact and what the characteristics of their interactions were.[56] Researchers continue to use this corpus to standardize the measurement of the effectiveness of their algorithms.[50][51][53]
Other algorithms identify drug-drug interactions from patterns in user-generated content, especially electronic health records and/or adverse event reports.[51][52] Organizations such as the FDA Adverse Event Reporting System (FAERS) and the World Health Organization's VigiBase allow doctors to submit reports of possible negative reactions to medications. Deep learning algorithms have been developed to parse these reports and detect patterns that imply drug-drug interactions.[57]
Telemedicine
The increase of telemedicine, the treatment of patients remotely, has shown the rise of possible AI applications.[58] AI can assist in caring for patients remotely by monitoring their information through sensors.[59] A wearable device may allow for constant monitoring of a patient and the ability to notice changes that may be less distinguishable by humans. The information can be compared to other data that has already been collected using artificial intelligence algorithms that alert physicians if there are any issues to be aware of.[59]
A 2025 systematic review and meta-analysis of 15 studies comparing AI chatbots with human healthcare professionals in text-based consultations found that in a large majority of studies participants rated chatbot responses as more empathic than those from clinicians.[60]
Another application of artificial intelligence is chat-bot therapy. Some researchers charge that the reliance on chatbots for mental healthcare does not offer the reciprocity and accountability of care that should exist in the relationship between the consumer of mental healthcare and the care provider (be it a chat-bot or psychologist), though.[61] Some examples of these chatbots include Woebot, Earkick and Wysa.[62][63][64]
Since the average age has risen due to a longer life expectancy, artificial intelligence could be useful in helping take care of older populations.[65] Tools such as environment and personal sensors can identify a person's regular activities and alert a caretaker if a behavior or a measured vital is abnormal.[65] Although the technology is useful, there are also discussions about limitations of monitoring in order to respect a person's privacy since there are technologies that are designed to map out home layouts and detect human interactions.[65]
Workload management
AI has the potential to streamline care coordination and reduce the workload. AI algorithms can automate administrative tasks, prioritize patient needs, and facilitate seamless communication in a healthcare team.[66]
Clinical applications
Cardiovascular
Artificial intelligence algorithms have shown promising results in accurately diagnosing and risk stratifying patients with concern for coronary artery disease, showing potential as an initial triage tool.[67][68] Other algorithms have been used in predicting patient mortality, medication effects, and adverse events following treatment for acute coronary syndrome.[67] Wearables, smartphones, and internet-based technologies have also shown the ability to monitor patients' cardiac data points, expanding the amount of data and the various settings AI models can use and potentially enabling earlier detection of cardiac events occurring outside of the hospital.[69] A study in 2019 found that AI can be used to predict heart attack with up to 90% accuracy.[70] Another growing area of research is the utility of AI in classifying heart sounds and diagnosing valvular disease.[71] Challenges of AI in cardiovascular medicine have included the limited data available to train machine learning models, such as limited data on social determinants of health as they pertain to cardiovascular disease.[72]
A key limitation in early studies evaluating AI were omissions of data comparing algorithmic performance to humans. Examples of studies which assess AI performance relative to physicians includes how AI is non-inferior to humans in interpretation of cardiac echocardiograms[73] and that AI can diagnose heart attack better than human physicians in the emergency setting, reducing both low-value testing and missed diagnoses.[74]
In cardiovascular tissue engineering and organoid studies, AI is increasingly used to analyze microscopy images, and integrate electrophysiological read outs.[75]
Han et al. showed keratinocytic skin cancer detection from face photographs.[77] Esteva et al. demonstrated dermatologist-level classification of skin cancer from lesion images.[78] Noyan et al. demonstrated a convolutional neural network that achieved 94% accuracy at identifying skin cells from microscopic Tzanck smear images.[79] Concerns have been raised, however, regarding the limited diversity of datasets, particularly the underrepresentation of darker skin tones, which may reduce generalizability across populations.[80]
In addition to skin cancer detection and analysis of tissue samples of histological smears, AI has been used in chronic and aesthetic dermatology.[81]
MDalgorithms has developed a mobile application MDacne which uses machine learning to grade acne severity from smartphone selfies and generate treatment regimens.[82] AI has also been used to diagnose inflammatory skin conditions such as rosacea, where an AI tool was reported to achieve accuracy rates of approximately 88–90% in identifying the disorder.[83] MDhair applies AI analysis to scalp photographs to personalize hair loss treatments, with clinical trials reporting reductions in shedding, increased density, and improved scalp hydration.[84]
A large study involving over one million individuals describes the use of AI-based systems in collecting demographic and clinical data on skin and hair health, enabling the identification of population-level trends.[85]
According to some researchers, AI algorithms have been shown to be more effective than dermatologists at identifying cancer.[86] However, a 2021 review article found that a majority of papers analyzing the performance of AI algorithms designed for skin cancer classification failed to use external test sets.[87] Only four research studies were found in which the AI algorithms were tested on clinics, regions, or populations distinct from those it was trained on, and in each of those four studies, the performance of dermatologists was found to be on par with that of the algorithm. Moreover, only one study[88] was set in the context of a full clinical examination; others were based on interaction through web-apps or online questionnaires, with most based entirely on context-free images of lesions. In this study, it was found that dermatologists significantly outperformed the algorithms. Many articles claiming superior performance of AI algorithms also fail to distinguish between trainees and board-certified dermatologists in their analyses.[87]
It has also been suggested that AI could be used to automatically evaluate the outcome of maxillo-facial surgery or cleft palate therapy in regard to facial attractiveness or age appearance.[89][90]
Gastroenterology
AI can play a role in various facets of the field of gastroenterology. Endoscopic exams such as esophagogastroduodenoscopies (EGD) and colonoscopies rely on rapid detection of abnormal tissue. By enhancing these endoscopic procedures with AI, clinicians can more rapidly identify diseases, determine their severity, and visualize blind spots. Early trials in using AI detection systems of early stomach cancer have shown sensitivity close to expert endoscopists.[91]
AI can assist doctors treating ulcerative colitis in detecting the microscopic activity of the disease in people and predicting when flare-ups will happen. For example, an AI-powered tool was developed to analyse digitised bowel samples (biopsies). The tool was able to distinguish with 80% accuracy between samples that show remission of colitis and those with active disease. It also predicted the risk of a flare-up happening with the same accuracy. These rates of successfully using microscopic disease activity to predict disease flare are similar to the accuracy of pathologists.[92][93]
Infectious diseases
AI has shown potential in both the laboratory and clinical spheres of infectious disease medicine.[94] During the COVID-19 pandemic, AI has been used for early detection, tracking virus spread and analysing virus behaviour, among other things.[95] However, there were only a few examples of AI being used directly in clinical practice during the pandemic itself.[96]
AI has been used to identify causes of knee pain that doctors miss, that disproportionately affect Black patients.[97] Underserved populations experience higher levels of pain. These disparities persist even after controlling for the objective severity of diseases like osteoarthritis, as graded by human physicians using medical images, raising the possibility that underserved patients' pain stems from factors external to the knee, such as stress. Researchers have conducted a study using a machine-learning algorithm to show that standard radiographic measures of severity overlook objective but undiagnosed features that disproportionately affect diagnosis and management of underserved populations with knee pain. They proposed that new algorithmic measure ALG-P could potentially enable expanded access to treatments for underserved patients.[98]
Neurology
The use of AI technologies has been explored for use in the diagnosis and prognosis of Alzheimer's disease (AD). For diagnostic purposes, machine learning models have been developed that rely on structural MRI inputs.[99] The input datasets for these models are drawn from databases such as the Alzheimer's Disease Neuroimaging Initiative.[100] Researchers have developed models that rely on convolutional neural networks with the aim of improving early diagnostic accuracy.[101]Generative adversarial networks are a form of deep learning that have also performed well in diagnosing AD.[102] There have also been efforts to develop machine learning models into forecasting tools that can predict the prognosis of patients with AD. Forecasting patient outcomes through generative models has been proposed by researchers as a means of synthesizing training and validation sets.[103] They suggest that generated patient forecasts could be used to provide future models larger training datasets than current open access databases.
Oncology
AI has been explored for use in cancer diagnosis, risk stratification, molecular characterization of tumors, and cancer drug discovery.[104] A particular challenge in oncologic care that AI is being developed to address is the ability to accurately predict which treatment protocols will be best suited for each patient based on their individual genetic, molecular, and tumor-based characteristics.[105] AI has been trialed in cancer diagnostics with the reading of imaging studies and pathology slides.[106]
In January 2020, Google DeepMind announced an algorithm capable of surpassing human experts in breast cancer detection in screening scans.[107][108] A number of researchers, including Trevor Hastie, Joelle Pineau, and Robert Tibshirani among others, published a reply claiming that DeepMind's research publication in Nature lacked key details on methodology and code, "effectively undermin[ing] its scientific value" and making it impossible for the scientific community to confirm the work.[109] In the MIT Technology Review, author Benjamin Haibe-Kains characterized DeepMind's work as "an advertisement" having little to do with science.[110]
In July 2020, it was reported that an AI algorithm developed by the University of Pittsburgh achieves the highest accuracy to date in identifyingprostate cancer, with 98% sensitivity and 97% specificity.[111][112] In 2023 a study reported the use of AI for CT-based radiomics classification at grading the aggressiveness of retroperitoneal sarcoma with 82% accuracy compared with 44% for lab analysis of biopsies.[113][114]
Ophthalmology
Artificial intelligence-enhanced technology is being used as an aid in the screening of eye disease and prevention of blindness.[115] In 2018, the U.S. Food and Drug Administration authorized the marketing of the first medical device to diagnose a specific type of eye disease, diabetic retinopathy using an artificial intelligence algorithm.[116] Moreover, AI technology may be used to further improve "diagnosis rates" because of the potential to decrease detection time.[117]
Ki67 stain calculation by the open-source software QuPath in a pure seminoma, which gives a measure of the proliferation rate of the tumor. The colors represent the intensity of expression: blue-no expression, yellow-low, orange-moderate, and red-high expression.
For many diseases, pathological analysis of cells and tissues is considered to be the gold standard of disease diagnosis. Methods of digital pathology allow microscopy slides to be scanned and digitally analyzed. AI-assisted pathology tools have been developed to assist with the diagnosis of a number of diseases, including breast cancer, hepatitis B, gastric cancer, and colorectal cancer. AI has also been used to predict genetic mutations and prognosticate disease outcomes.[91] AI is well-suited for use in low-complexity pathological analysis of large-scale screening samples, such as colorectal or breast cancer screening, thus lessening the burden on pathologists and allowing for faster turnaround of sample analysis.[119] Several deep learning and artificial neural network models have shown accuracy similar to that of human pathologists,[119] and a study of deep learning assistance in diagnosing metastatic breast cancer in lymph nodes showed that the accuracy of humans with the assistance of a deep learning program was higher than either the humans alone or the AI program alone.[120] Additionally, implementation of digital pathology is predicted to save over $12 million for a university center over the course of five years,[121] though savings attributed to AI specifically have not yet been widely researched. The use of augmented and virtual reality could prove to be a stepping stone to wider implementation of AI-assisted pathology, as they can highlight areas of concern on a pathology sample and present them in real-time to a pathologist for more efficient review.[119] AI also has the potential to identify histological findings at levels beyond what the human eye can see,[119] and has shown the ability to use genotypic and phenotypic data to more accurately detect the tumor of origin for metastatic cancer.[122] One of the major current barriers to widespread implementation of AI-assisted pathology tools is the lack of prospective, randomized, multi-center controlled trials in determining the true clinical utility of AI for pathologists and patients, highlighting a current area of need in AI and healthcare research.[119]
In pharmacy, AI helps discover, develop and deliver medications, and can enhance patient care through personalized treatment plans.[123][124]
Primary care
Primary care has become one key development area for AI technologies.[125][126] AI in primary care has been used for supporting decision making, predictive modeling, and business analytics.[127] There are only a few examples of AI decision support systems that were prospectively assessed on clinical efficacy when used in practice by physicians. But there are cases where the use of these systems yielded a positive effect on treatment choice by physicians.[128]
As of 2022 in relation to elder care, AI robots had been helpful in guiding older residents living in assisted living with entertainment and company. These bots are allowing staff in the home to have more one-on-one time with each resident, but the bots are also programmed with more ability in what they are able to do; such as knowing different languages and different types of care depending on the patient's conditions. The bot is an AI machine, which means it goes through the same training as any other machine - using algorithms to parse the given data, learn from it and predict the outcome in relation to what situation is at hand.[129]
Psychiatry and psychology
People have used AI chatbots such as ChatGPT as a replacement for therapy when such therapy is unaffordable or inaccessible. Chatbots used for this purpose lack boundaries and are unregulated. This can lead to a risk of unhealthy attachment from users and coincides with chatbot psychosis. AI chatbots, including those used as a substitute for therapy, have provided harmful advice which has led to death. This has led to some government and institutional efforts to regulate or outlaw chatbot therapy.[130][131][132][133]
Chatbots have been studied as a way to treat anxiety and depression.[134] Although AI applications have been developed and proposed for screening for suicidal ideation, legal and privacy issues and public opposition has limited implementation.[135][136] Small training datasets contain bias that is inherited by the models, and compromises the generalizability and stability of these models. Such models may also have the potential to be discriminatory against minority groups that are underrepresented in samples.[137]
AI is being studied within the field of radiology to detect and diagnose diseases through computerized tomography (CT) and magnetic resonance (MR) imaging.[141] It may be particularly useful in settings where demand for human expertise exceeds supply, or where data is too complex to be efficiently interpreted by human readers.[142] Several deep learning models have shown the capability to be roughly as accurate as healthcare professionals in identifying diseases through medical imaging, though few of the studies reporting these findings have been externally validated.[143] AI can also provide non-interpretive benefit to radiologists, such as reducing noise in images, creating high-quality images from lower doses of radiation, enhancing MR image quality,[144] and automatically assessing image quality.[145] Further research investigating the use of AI in nuclear medicine focuses on image reconstruction, anatomical landmarking, and the enablement of lower doses in imaging studies.[146] The analysis of images for supervised AI applications in radiology encompasses two primary techniques at present: (1) convolutional neural network-based analysis; and (2) utilization of radiomics.[142]
AI is also used in breast imaging for analyzing screening mammograms and can participate in improving breast cancer detection rate[147] as well as reducing radiologist's reading workload.
As of 2025, 77% (967 out of 1247) of all FDA-approved AI-enabled medical devices are in radiology.[148]
Industry
The trend of large health companies merging has allowed for greater health data accessibility. Greater health data have laid the groundwork to implement AI algorithms.
A large part of industry focus has been in the clinical decision support systems. As more data is collected, machine learning algorithms adapt and allow for more robust responses and solutions.[141] Numerous companies have been exploring the possibilities of the incorporation of big data in the healthcare industry, many of whom have been investigating market opportunities through "data assessment, storage, management, and analysis technologies".[149] With the market for AI expanding, large tech companies such as Apple, Google, Amazon, and Baidu all have their own AI research divisions, as well as millions of dollars allocated for acquisition of smaller AI based companies.[149]
Large companies
The following are examples of large companies that are contributing to AI algorithms for use in healthcare:
Intel's venture capital arm Intel Capital invested in 2016 in the startup Lumiata, which uses AI to identify at-risk patients and develop care options.[150]
Siemens Healthineers applies AI in imaging and diagnostics, including algorithms to reconstruct CT images and guide ultrasound procedures. It also uses AI to support treatment planning such as radiation therapy for cancer, improve point-of-care diagnostics, and automate lab workflows.[151]
Microsoft's Hanover project, in partnership with Oregon Health & Science University's Knight Cancer Institute, analyzes medical research to predict the most effective cancer drug treatment options for patients. Other projects include medical image analysis of tumor progression and the development of programmable cells.[152]
Philips Healthcare develops AI-powered diagnostic tools that analyze medical images to detect subtle anomalies. Its AI technologies also support precision oncology by assisting pathologists in cancer diagnosis, care management, and patient monitoring.[153]
Smaller companies, applications
Elon Musk premiering the surgical robot that implants the Neuralink brain chip
Neuralink has come up with a next-generation neuroprosthetic which intricately interfaces with thousands of neural pathways in the brain.[141] Their process allows a chip, roughly the size of a quarter, to be inserted in the place of a chunk of a skull by a precision surgical robot to avoid accidental injury.[141]
Tencent has been working on several medical systems and services. These include AI Medical Innovation System (AIMIS), an AI-powered diagnostic medical imaging service; WeChat Intelligent Healthcare; and Tencent Doctorwork[154]
The Indian startup Haptik developed a WhatsApp chatbot in 2021 which answered questions associated with COVID-19 in India. Similarly, a software platform ChatBot in partnership with health technology startup Infermedica launched COVID-19 Risk Assessment ChatBot.[157]
In 2021, Accofrisk AI Health was launched in China as an artificial intelligence–based platform for remote and non-invasive health monitoring. The AI creates digital health twins of users, tracks over 300 physical and mental health parameters, assesses disease risks, and supports data analysis for health-related decision-making. As of 2026, the platform is connected to 1,000,000 users, including company employees and clinic patients.
Expanding care to developing nations
Artificial intelligence continues to expand in its abilities to diagnose more people accurately in nations where fewer doctors are accessible to the public. Many new technology companies such as SpaceX and the Raspberry Pi Foundation have enabled more developing countries to have access to computers and the internet than ever before.[158] With the increasing capabilities of AI over the internet, advanced machine learning algorithms can allow patients to get accurately diagnosed when they would previously have no way of knowing if they had a life-threatening disease or not.[158]
Using AI in developing nations that do not have the resources will diminish the need for outsourcing and can improve patient care. AI can allow for not only diagnosis of patient in areas where healthcare is scarce, but also allow for a good patient experience by resourcing files to find the best treatment for a patient.[159] The ability of AI to adjust course as it goes also allows the patient to have their treatment modified based on what works for them; a level of individualized care that is nearly non-existent in developing countries.[159]
Regulation
This section needs to be updated. Please help update this article to reflect recent events or newly available information.(May 2025)
Challenges of the clinical use of AI have brought about a potential need for regulations. AI studies need to be completely and transparently reported to have value to inform regulatory approval. Depending on the phase of study, international consensus-based reporting guidelines (TRIPOD+AI,[160] DECIDE-AI,[161] CONSORT-AI[162]) have been developed to provide recommendations on the key details that need to be reported.
A man speaking at the GDPR compliance workshop at the 2019 Entrepreneurship Summit
While regulations exist pertaining to the collection of patient data such as the Health Insurance Portability and Accountability Act in the US (HIPAA) and the European General Data Protection Regulation (GDPR) pertaining to patients within the EU, health care AI is "severely under-regulated worldwide" as of 2025.[163] Unclear is whether healthcare AI can be classified merely as software or as medical device.[163]
United Nations (WHO/ITU)
The ITU-WHO Focus Group on Artificial Intelligence for Health (FG-AI4H) has built a platform known as the ITU-WHO AI for Health Framework for the testing and benchmarking of AI applications in health domain as a joint endeavor of ITU and WHO. As of November 2018, eight use cases were being benchmarked, including assessing breast cancer risk from histopathological imagery, guiding anti-venom selection from snake images, and diagnosing skin lesions.
USA
United States Food & Drug Administration
In 2015, the Office for Civil Rights (OCR) issued rules and regulations to protect the privacy of individuals' health information, requiring healthcare providers to follow certain privacy rules when using AI, to keep a record of how they use AI and to ensure that their AI systems are secure.[165]
In May 2016, the White House announced its plan to host a series of workshops and formation of the National Science and Technology Council (NSTC) Subcommittee on Machine Learning and Artificial Intelligence.[166][167] In October 2016, the group published The National Artificial Intelligence Research and Development Strategic Plan, outlining its proposed priorities for Federally-funded AI research and development (within government and academia). The report notes a strategic R&D plan for the subfield of health information technology was in development stages.[167]
In January 2021, the US FDA published a new Action Plan, entitled Artificial Intelligence (AI) /Machine Learning (ML)-Based Software as a Medical Device (SaMD) Action Plan.[168] It laid out the FDA's future plans for regulation of medical devices that would include artificial intelligence in their software with five main actions: 1. Tailored Regulatory Framework for Ai/M:-based SaMD, 2. Good Machine Learning Practice (GMLP), 3. Patient-Centered Approach Incorporating Transparency to Users, 4. Regulatory Science Methods Related to Algorithm Bias & Robustness, and 5. Real-World Performance(RWP). This plan was in direct response to stakeholders' feedback on a 2019 discussion paper also published by the FDA.[168]
Under President Biden the DHSS and the National Institute of Standards and Technology were instructed to develop regulation of healthcare AI.[163] According to the U.S. Department of Health and Human Services, the OCR issued guidance on the ethical use of AI in healthcare in 2021. It outlined four core ethical principles that must be followed: respect for autonomy, beneficence, non-maleficence, and justice. Respect for autonomy requires that individuals have control over their own data and decisions. Beneficence requires that AI be used to do good, such as improving the quality of care and reducing health disparities. Non-maleficence requires that AI be used to do no harm, such as avoiding discrimination in decisions. Finally, justice requires that AI be used fairly, such as using the same standards for decisions no matter a person's race, gender, or income level. As of March 2021, the OCR had hired a Chief Artificial Intelligence Officer (OCAIO) to pursue the "implementation of the HHS AI strategy".[169]
With the second Trump administration deregulation of health AI began on January 20, 2025 with merely voluntary standards for collecting and sharing data, statutory definitions for algorithmic discrimination, automation bias, and equity being cancelled, cuts to NIST and 19% of FDA workforce eliminated.[163]
Europe
Other countries have implemented data protection regulations, more specifically with company privacy invasions. In Denmark, the Danish Expert Group on data ethics has adopted recommendations on "Data for the Benefit of the People". These recommendations are intended to encourage the responsible use of data in the business sector, with a focus on data processing. The recommendations include a focus on equality and non-discrimination with regard to bias in AI, as well as human dignity which is to outweigh profit and must be respected in all data processes.[170]
The European Union has implemented the General Data Protection Regulation (GDPR) to protect citizens' personal data, which applies to the use of AI in healthcare. In addition, the European Commission has established guidelines to ensure the ethical development of AI, including the use of algorithms to ensure fairness and transparency.[171] With GDPR, the European Union was the first to regulate AI through data protection legislation. The Union finds privacy as a fundamental human right, it wants to prevent unconsented and secondary uses of data by private or public health facilities. By streamlining access to personal data for health research and findings, they are able to instate the right and importance of patient privacy.[171]
In March 2024, the European Union approved the pivotal Artificial Intelligence Act (AI Act).[172] The regulation applies to European companies and organizations, and foreign providers of AI systems in the EU market. The EU AI Act has a risk-based structure, where AI enabled medical devices are in the "high-risk" category, the highest risk category of permitted uses for AI.[172]
In the United States, the Health Insurance Portability and Accountability Act (HIPAA) requires organizations to protect the privacy and security of patient information. The Centers for Medicare and Medicaid Services have also released guidelines for the development of AI-based medical applications.[173]
In 2025, Europe was leading the USA on AI regulation, while lagging in innovation and at least one California-based biotech company was "engaging the European Medicines Agency earlier in development than previously anticipated to mitigate concerns about the FDA's ability to meet development timelines."[163]
Ethical concerns
While research on the use of AI in healthcare aims to validate its efficacy in improving patient outcomes before its broader adoption, its use may introduce several new types of risk to patients and healthcare providers, such as algorithmic bias, Do not resuscitate implications, and other machine morality issues. AI may also compromise the protection of patients' rights, such as the right to informed consent and the right to medical data protection.[174]
Privacy and data collection
In order to effectively train machine learning systems and use them in healthcare, massive amounts of data must be gathered. Acquiring this data, however, comes at the cost of patient privacy, which can be controversial. For example, a survey conducted in the UK estimated that 63% of the population is uncomfortable with sharing their personal data in order to improve AI technology.[175] The scarcity of real, accessible patient data is a hindrance that deters the progress of developing and deploying more AI in healthcare.
The lack of regulations surrounding AI in the United States has generated concerns about mismanagement of patient data, such as with corporations utilizing patient data for financial gain. For example, as of 2020, the Swiss healthcare company Roche reportedly purchased healthcare data for approximately 2 million cancer patients at an estimated total cost of $1.9 billion.[176] This generated ethical concerns about whether it was fair to sell patients' data, even considering the benefits. Ultimately, the current potential of AI in healthcare is additionally hindered by concerns about mismanagement of data collected, especially in the United States.
The use of large language models for healthcare consultations introduces particular privacy risks, such as increased exposure of sensitive health information during consultations that may be collected for model retraining. A 2024 study of 846 Chinese users found that while 77.3% expressed willingness to use LLM-based healthcare services, privacy awareness varied significantly by demographics and cultural context.[177] The research revealed a "privacy paradox" where users who claimed greater privacy knowledge and concern actually showed higher acceptance of information sharing, potentially due to better understanding of legitimate uses such as academic research and service improvement.[178]
Privacy expectations for LLMs vary significantly across cultural contexts. Research in China has shown that users may have different privacy norms compared to Western populations, with factors such as age, education level, and medical background influencing acceptance of data sharing. Younger and more educated users tend to be more privacy-conscious, while those with medical backgrounds show greater acceptance of health data sharing for legitimate medical purposes.[178]
A systematic review and thematic analysis in 2023 showed that most stakeholders including health professionals, patients, and the general public doubted that care involving AI could be empathetic, or fulfill beneficence.[17]
According to a 2019 study, AI can replace up to 35% of jobs in the UK within the next 10 to 20 years.[179] However, of these jobs, it was concluded that AI has not eliminated any healthcare jobs so far. Though if AI were to automate healthcare-related jobs, the jobs most susceptible to automation would be those dealing with digital information, radiology, and pathology, as opposed to those dealing with doctor-to-patient interaction.[179]
Outputs can be incorrect or incomplete and diagnosis and recommendations harm people.[163]
Bias and discrimination
Since AI makes decisions solely on the data it receives as input, it is important that this data represents accurate patient demographics. In a hospital setting, patients do not have full knowledge of how predictive algorithms are created or calibrated. Therefore, these medical establishments can unfairly code their algorithms to discriminate against minorities and prioritize profits rather than providing optimal care, i.e. violating the ethical principle of social justice or non-maleficence.[180] A recent scoping review identified 18 equity challenges along with 15 strategies that can be implemented to help address them when AI applications are developed using many-to-many mapping.[181]
There can be unintended bias in algorithms that can exacerbate social and healthcare inequities.[180] Since AI's decisions are a direct reflection of its input data, the data it receives must have accurate representation of patient demographics. For instance, if populations are less represented in healthcare data it is likely to create bias in AI tools that lead to incorrect assumptions of a demographic and impact the ability to provide appropriate care.[182] White males are overly represented in medical data sets.[183] Therefore, having minimal patient data on minorities can lead to AI making more accurate predictions for majority populations, leading to unintended worse medical outcomes for minority populations.[184] Collecting data from minority communities can also lead to medical discrimination. For instance, HIV is a prevalent virus among minority communities and HIV status can be used to discriminate against patients.[183] In addition to biases that may arise from sample selection, different clinical systems used to collect data may also impact AI functionality. For example, radiographic systems and their outcomes (e.g., resolution) vary by provider. Moreover, clinician work practices, such as the positioning of the patient for radiography, can also greatly influence the data and make comparability difficult.[185] However, these biases are able to be eliminated through careful implementation and a methodical collection of representative data.
A final source of algorithmic bias, which has been called "label choice bias", arises when proxy measures are used to train algorithms, that build in bias against certain groups. For example, a widely used algorithm predicted health care costs as a proxy for health care needs, and used predictions to allocate resources to help patients with complex health needs. This introduced bias because Black patients have lower costs, even when they are just as unhealthy as White patients.[186] Solutions to the "label choice bias" aim to match the actual target (what the algorithm is predicting) more closely to the ideal target (what researchers want the algorithm to predict), so for the prior example, instead of predicting cost, researchers would focus on the variable of healthcare needs which is rather more significant. Adjusting the target led to almost double the number of Black patients being selected for the program.
History
Research in the 1960s and 1970s produced the first problem-solving program, or expert system, known as Dendral.[187][188] While it was designed for applications in organic chemistry, it provided the basis for a subsequent system MYCIN,[189] considered one of the most significant early uses of artificial intelligence in medicine.[189][190] MYCIN and other systems such as INTERNIST-1 and CASNET did not achieve routine use by practitioners, however.[191]
The 1980s and 1990s brought the proliferation of the microcomputer and new levels of network connectivity. During this time, there was a recognition by researchers and developers that AI systems in healthcare must be designed to accommodate the absence of perfect data and build on the expertise of physicians.[192] Approaches involving fuzzy set theory,[193]Bayesian networks,[194] and artificial neural networks,[195][196] have been applied to intelligent computing systems in healthcare.
Medical and technological advancements occurring over this half-century period that have enabled the growth of healthcare-related applications of AI to include:
↑Lyakhova UA, Lyakhov PA (August 2024). "Systematic review of approaches to detection and classification of skin cancer using artificial intelligence: Development and prospects". Computers in Biology and Medicine. 178 108742. doi:10.1016/j.compbiomed.2024.108742. PMID38875908.
↑Matthew B. A. McDermott, etal. (March 24, 2021). "Reproducibility in machine learning for health research: Still a ways to go". Science Translational Medicine. 13 (586) eabb1655. doi:10.1126/scitranslmed.abb1655. PMID33762434.
↑Garza-Galicia, M., Sosa, M., Low, R., & Simini, F. (2017). Enseñanza de un Programa de Ortesis Mental Clínica: Experiencia con Estudiantes de Medicina en Uruguay. Memorias Del Congreso Nacional De Ingeniería Biomédica, 4(1), 91–94. Retrieved from: http://memorias.somib.org.mx/index.php/memorias/article/view/221Archived 2021-08-13 at the Wayback Machine
123Eren A, Subasi A, Coskun O (February 2008). "A decision support system for telemedicine through the mobile telecommunications platform". Journal of Medical Systems. 32 (1): 31–35. doi:10.1007/s10916-007-9104-x. PMID18333403. S2CID11082133.
↑Bennett CC, Doub TW, Selove R (April 2012). "EHRs connect research and practice: Where predictive modeling, artificial intelligence, and clinical decision support intersect". Health Policy and Technology. 1 (2): 105–114. arXiv:1204.4927. doi:10.1016/j.hlpt.2012.03.001. ISSN2211-8837. S2CID25022446.
↑Blease C, Locher C, Leon-Carlyle M, Doraiswamy M (January 2020). "Artificial intelligence and the future of psychiatry: Qualitative findings from a global physician survey". DIGITAL HEALTH. 6. doi:10.1177/2055207620968355.
↑Kharko A, Locher C, Torous J, Rosch SA, Hägglund M, Gaab J, etal. (July 2025). "Generative artificial intelligence in medicine: a mixed-methods survey of UK general practitioners". BMJ Digital Health & AI. 1 (1) e000051. doi:10.1136/bmjdhai-2025-000051.
↑Kharko A, McMillan B, Hagström J, Muli I, Davidge G, Hägglund M, etal. (January 2024). "Generative artificial intelligence writing open notes: A mixed methods assessment of the functionality of GPT 3.5 and GPT 4.0". DIGITAL HEALTH. 10. doi:10.1177/20552076241291384.
↑Ayers JW, Poliak A, Dredze M, Leas EC, Zhu Z, Kelley JB, etal. (1 June 2023). "Comparing Physician and Artificial Intelligence Chatbot Responses to Patient Questions Posted to a Public Social Media Forum". JAMA Internal Medicine. 183 (6): 589. doi:10.1001/jamainternmed.2023.1838.
↑Kharko A, McMillan B, Hagström J, Muli I, Davidge G, Hägglund M, etal. (January 2024). "Generative artificial intelligence writing open notes: A mixed methods assessment of the functionality of GPT 3.5 and GPT 4.0". DIGITAL HEALTH. 10. doi:10.1177/20552076241291384.
↑Baker HP, Dwyer E, Kalidoss S, Hynes K, Wolf J, Strelzow JA (1 February 2024). "ChatGPT's Ability to Assist with Clinical Documentation: A Randomized Controlled Trial". Journal of the American Academy of Orthopaedic Surgeons. 32 (3): 123–129. doi:10.5435/JAAOS-D-23-00474.
↑Kharko A, McMillan B, Hagström J, Muli I, Davidge G, Hägglund M, etal. (January 2024). "Generative artificial intelligence writing open notes: A mixed methods assessment of the functionality of GPT 3.5 and GPT 4.0". DIGITAL HEALTH. 10. doi:10.1177/20552076241291384.
↑Blease C, Torous J (November 2023). "ChatGPT and mental healthcare: balancing benefits with risks of harms". BMJ Mental Health. 26 (1) e300884. doi:10.1136/bmjment-2023-300884.
↑García JS (2013-04-14). Optimización del tratamiento de enfermos pluripatológicos en atención primaria UCAMI HHUU Virgen del Rocio (Report). Sevilla. Spain – via ponencias de la II Reunión de Paciente Pluripatológico y Edad Avanzada Archived.
↑Segura Bedmar I, Martínez P, Herrero Zazo M (June 2013). Semeval-2013 task 9: Extraction of drug-drug interactions from biomedical texts (ddiextraction 2013). Second Joint Conference on Lexical and Computational Semantics. Vol.2. Association for Computational Linguistics. pp.341–350.
↑Hamet P, Tremblay J (April 2017). "Artificial intelligence in medicine". Metabolism. Insights Into the Future of Medicine: Technologies, Concepts, and Integration. 69S: S36–S40. doi:10.1016/j.metabol.2017.01.011. PMID28126242.
↑Stokes F, Palmer A (October 2020). "Artificial Intelligence and Robotics in Nursing: Ethics of Caring as a Guide to Dividing Tasks Between AI and Humans". Nursing Philosophy. 21 (4) e12306. doi:10.1111/nup.12306. PMID32609420.
12Wang H, Zu Q, Chen J, Yang Z, Ahmed MA (October 2021). "Application of Artificial Intelligence in Acute Coronary Syndrome: A Brief Literature Review". Advances in Therapy. 38 (10): 5078–5086. doi:10.1007/s12325-021-01908-2. PMID34528221. S2CID237522871.
↑Hibler BP, Qi Q, Rossi AM (March 2016). "Current state of imaging in dermatology". Seminars in Cutaneous Medicine and Surgery. 35 (1): 2–8. doi:10.12788/j.sder.2016.001 (inactive 1 July 2025). PMID26963110.{{cite journal}}: CS1 maint: DOI inactive as of July 2025 (link)
↑Patcas R, Timofte R, Volokitin A, Agustsson E, Eliades T, Eichenberger M, etal. (August 2019). "Facial attractiveness of cleft patients: a direct comparison between artificial-intelligence-based scoring and conventional rater groups". European Journal of Orthodontics. 41 (4): 428–433. doi:10.1093/ejo/cjz007. hdl:20.500.11850/377316. PMID30788496. S2CID73507799.
↑Mishra A, Sharma S, Pandey SK (2025-02-03). "The Present State and Potential Applications of Artificial Intelligence in Cancer Diagnosis and Treatment". Recent Patents on Anti-Cancer Drug Discovery. 20 (3): 287–305. doi:10.2174/0115748928361472250123105507. ISSN2212-3970. PMID39902536.
↑Coppersmith G, Leary R, Crutchley P, Fine A (January 2018). "Natural Language Processing of Social Media as Screening for Suicide Risk". Biomedical Informatics Insights. 10 1178222618792860. doi:10.1177/1178222618792860. PMC6111391. PMID30158822. We examined the ethical and privacy concerns around the use of these algorithms for screening and monitoring, concluding that there are novel ways to consider using information from these algorithms to aid intervention, but the general public has voiced opposition to related approaches. Although the design of an intervention system powered by algorithmic screening is technically possible, the cultural implications of implementation are far from settled.
↑Richardson ML, Garwood ER, Lee Y, Li MD, Lo HS, Nagaraju A, etal. (September 2021). "Noninterpretive Uses of Artificial Intelligence in Radiology". Academic Radiology. 28 (9): 1225–1235. doi:10.1016/j.acra.2020.01.012. PMID32059956.
↑Seifert R, Weber M, Kocakavuk E, Rischpler C, Kersting D (March 2021). "Artificial Intelligence and Machine Learning in Nuclear Medicine: Future Perspectives". Seminars in Nuclear Medicine. 51 (2): 170–177. doi:10.1053/j.semnuclmed.2020.08.003. PMID33509373. S2CID224863373.
12Abou-Zahra S, Brewer J, Cooper M (2018-04-23). "Artificial Intelligence (AI) for Web Accessibility". Proceedings of the 15th International Web for All Conference. W4A '18. Lyon, France: Association for Computing Machinery. pp.1–4. doi:10.1145/3192714.3192834. ISBN978-1-4503-5651-0. S2CID49863409.
↑Lacassie E, Marquet P, Martin-Dupont S, Gaulier JM, Lachâtre G (September 2000). "A non-fatal case of intoxication with foxglove, documented by means of liquid chromatography-electrospray-mass spectrometry". Journal of Forensic Sciences. 45 (5): 1154–1158. doi:10.1520/JFS14845J. PMID11005196.
12Liu Z, Hu L, Zhou T, Tang Y, Cai Z (May 2025). "Prevalence Overshadows Concerns? Understanding Chinese Users' Privacy Awareness and Expectations Towards LLM-Based Healthcare Consultation". 2025 IEEE Symposium on Security and Privacy (SP). pp.2716–2734. doi:10.1109/SP61157.2025.00092. ISBN979-8-3315-2236-0.
↑Lea AS (2023). Digitizing Diagnosis: Medicine, Minds, and Machines in Twentieth-Century America. Johns Hopkins University Press. pp.1–256. ISBN978-1-4214-4681-3.
12Clancey WJ, Shortliffe EH (1984). Readings in medical artificial intelligence: the first decade. Addison-Wesley Longman Publishing Co., Inc.
↑Bruce G, Buchanan BG, Shortliffe ED (1984). Rule-based expert systems: the MYCIN experiments of the Stanford Heuristic Programming Project.
↑Adlassnig KP (July 1980). "A fuzzy logical model of computer-assisted medical diagnosis". Methods of Information in Medicine. 19 (3): 141–148. doi:10.1055/s-0038-1636674. PMID6997678.
↑Baxt WG (December 1991). "Use of an artificial neural network for the diagnosis of myocardial infarction". Annals of Internal Medicine. 115 (11): 843–848. doi:10.7326/0003-4819-115-11-843. PMID1952470.
↑Maclin PS, Dempsey J, Brooks J, Rand J (February 1991). "Using neural networks to diagnose cancer". Journal of Medical Systems. 15 (1): 11–19. doi:10.1007/bf00993877. PMID1748845. S2CID10189561.
↑Koomey J, Berard S, Sanchez M, Wong H (March 2010). "Implications of historical trends in the electrical efficiency of computing". IEEE Annals of the History of Computing. 33 (3): 46–54. CiteSeerX10.1.1.323.9505. doi:10.1109/MAHC.2010.28. S2CID8305701.
Bennett CC, Doub TW, Selove R (June 2012). "EHRs connect research and practice: Where predictive modeling, artificial intelligence, and clinical decision support intersect". Health Policy and Technology. 1 (2): 105–14. arXiv:1204.4927. doi:10.1016/j.hlpt.2012.03.001. S2CID25022446.
Cho SM, Austin PC, Ross HJ, Abdel-Qadir H, Chicco D, Tomlinson G, etal. (August 2021). "Machine Learning Compared With Conventional Statistical Models for Predicting Myocardial Infarction Readmission and Mortality: A Systematic Review". The Canadian Journal of Cardiology. 37 (8). Elsevier: 1207–1214. doi:10.1016/j.cjca.2021.02.020. PMID33677098. S2CID232141652.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.