Several across the life course (e.g. less education, hearing loss, vision loss, physical inactivity, obesity, high cholesterol, hypertension, diabetes, smoking, excessive alcohol consumption, social isolation, air pollution, traumatic brain injury, depression)[3]
Addressing risk factors throughout the life course, e.g. preventing, reducing or treating hearing and vision loss, depression, head injury and vascular risk factors (e.g. cholesterol, diabetes), decreasing smoking, and maintaining physical activity and cognitive stimulation[3]
Although the greatest risk factor for developing dementia is aging, dementia is not a normal part of the aging process; many people aged 90 and above show no signs of dementia.[12] Risk factors, diagnosis and caregiving practices are influenced by cultural and socio-environmental factors.[16] Several risk factors for dementia, such as smoking and obesity, are modifiable by lifestyle changes.
Dementia is currently the seventh leading cause of death worldwide and has 10million new cases reported every year (approximately one every three seconds).[1] In the UK it is the leading cause of death.[17] It is one of the main causes of disabilities in those aged over 65.[18] There is no known cure for dementia.[19]Acetylcholinesterase inhibitors such as donepezil are often used in some dementia subtypes and may be beneficial in mild to moderate stages, but the overall benefit may be minor. There are many measures that can improve the quality of life of a person with dementia and their caregivers. Cognitive behavioral therapy may give some benefit for treating the associated symptoms of depression.[20]
Signs and symptoms
The signs and symptoms of dementia may vary depending on the underlying subtype, particularly in the early stages but at the end stage of all types they are similar.[21] Symptoms may be grouped into three areas: cognitive, neuropsychiatric (behavioral and psychological), and motor.[3]
The cognitive symptoms of dementia relate to the area of the brain affected. Typically this includes memory plus one other cognitive region commonly affecting language, attention, problem solving or perception and orientation.[6] Signs of dementia include wandering, and getting lost in a familiar neighborhood, using unusual words to refer to familiar objects, forgetting the name of a close family member or friend, forgetting old memories, forgetting to pay bills, and being unable to complete tasks independently.[6][22] The symptoms progress at a continuous rate over several stages.[21][9] Most types of dementia are slowly progressive with some deterioration of the brain well established before signs of the disorder become apparent.
Neuropsychiatric symptoms (NPS) are a major feature of dementia affecting more than 90% of all cases, at different stages.[23] They often present as first or early symptoms or syndromes that may reflect the subtype of dementia at issue.[24] For example, a study has found that the first symptoms as NPS of personality change, and disinhibition will relate to a diagnosis of frontotemporal dementia.[24]
The behavioral symptoms can include agitation, restlessness, inappropriate behavior, sexual disinhibition, and verbal or physical aggression.[6] Many of these symptoms may be improved by non-pharmacological measures with higher ranking interventions given as massage therapy, personally-tailored therapy, and animal-assisted therapy.[23]
Psychological symptoms can include depression, hallucinations (most often visual), delusions, apathy, and anxiety.[6] Also common are personality changes with the progression of dementia, such as increases in neuroticism (negativity), and a decline in conscientiousness.[25]
Motor symptoms and signs may include changes in gait, repetitive movements, parkinsonism, or seizures.[6] Changes in gait can be responsible for falls.[6] An inability to relax muscles, known as paratonia is an induced motor dysfunction that affects most people with dementia. Motor impairments are correlated with cognitive impairments, and are a main cause of disability and dependency.[26] In advanced dementia paratonia may lead to fixed postures with contracted muscles, which can lead to broken skin, and infection, and also cause pain on movement. This type of motor disorder is not the same as that found in Lewy body dementias.[26]
Stages
The course of dementia is often described in three major stages (early or mild, middle or moderate, and late or severe) that show a pattern of progressive cognitive and functional impairment.[27] Different scales used to assess the stage of dementia include the Global Deterioration Scale (GDS) that uses seven stages in the progression, with mild (early) dementia only appearing as stage 4.[28][27] Two other scales used in relation to GDS are the Brief Cognitive Rating Scale (BCRS),[29] and the Functional Assessment Staging Tool (FAST).[28] The BCRS is a quick assessment that coincides with the GDS. It uses five axes in assessment – concentration, memory (recent and past), orientation, functioning and self-care.[29] FAST places more emphasis on functioning in daily living.[28] Another scale used is the Clinical Dementia Rating (CDR) scale originally designed just for Alzheimer's, that evaluates six main areas including memory, judgement, problem-solving, and personal care.[28]
Prodromal
A prodromal stage is a stage of pre-dementia, and includes mild cognitive impairment (MCI) and mild behavioral impairment (MBI).[30] Signs and symptoms at the prodromal stage may be subtle, often only becoming apparent in hindsight.[31] The loss of the sense of smell (anosmia) is recognized as a long prodromal stage in both Alzheimer's and Parkinson's disease.[32]
In mild cognitive impairment, that progresses to a dementia subtype, changes in the person's brain have been happening for a long time, but the symptoms are just beginning to appear. These problems, however, are not severe enough to affect daily function. If and when they do, the diagnosis becomes one of a dementia subtype, such as minor neurocognitve disorder of Lewy body disease, for example. The person may have some memory problems and trouble finding words, but they can solve everyday problems and competently handle their life affairs.[33] During this stage, it is ideal to ensure that advance care planning has occurred to protect the person's wishes. Advance directives exist that are specific to people living with dementia.[34] These can be particularly helpful in addressing the decisions related to feeding which come with the progression of the illness.
Mild cognitive impairment has been relisted in both DSM-5 and ICD-11 as "mild neurocognitive disorders", i.e. milder forms of the major neurocognitive disorder (dementia) subtypes.[35] MCI does not always progress to dementia, and sometimes symptoms resolve.[12] But MCI may mark the tipping point between normal brain aging, and the pathological changes of dementia.[36]
Early
In the early or mild stage of dementia, symptoms become noticeable to other people. In addition, the symptoms begin to interfere with daily activities, and will register a score on a mini–mental state examination (MMSE). The MMSE scores from a maximum of 30 to 0. The exam consists of questions grouped into seven categories, each representing a different cognitive domain – orientation to time, orientation to place, registering of three words, attention and calculation, recall of three words, language, and visual construction. A decline of two to four points is considered a reliable change, and about three points is also the expected annual decline.[37]
The symptoms of early dementia usually include memory difficulty, but can also include some word-finding problems, and problems with executive functions of planning and organization.[38] Managing finances may prove difficult. Other signs might be getting lost in new places, repeating things, and personality changes.[39] In some types of dementia, such as dementia with Lewy bodies and frontotemporal dementia, personality changes and difficulty with organization and planning may be the first signs.[40]
Middle
In the middle or moderate stage, dementia progresses with the worsening of initial symptoms. The rate of decline is different for each person. MMSE scores between 6 and 17 signal moderate dementia. For example, people with moderate Alzheimer's dementia lose almost all new information. People with dementia may be severely impaired in solving problems, and their social judgment is often impaired. They cannot usually function outside their own home, and generally should not be left alone. They may be able to do simple chores around the house but not much else, and begin to require assistance for personal care and hygiene beyond simple reminders.[41] In neurodegenerative demantias a lack of insight into having the condition will become evident.[42]
Late
People with late-stage, or severe dementia typically turn increasingly inward and need assistance with most or all of their personal care. 24 hour supervision to meet basic needs and ensure personal safety is usually needed. If left unsupervised, they may wander or fall; may not recognize common dangers such as a hot stove; or may not realize that they need to use the bathroom and become incontinent. Incontinence both urinary and fecal may become prominent features that can prove challenging for both the person affected and the caregiver.[43] They may not want to get out of bed, or may need assistance doing so. They may also struggle to walk.[44] Commonly, the person no longer recognizes familiar faces. They may have significant changes in sleeping habits or have trouble sleeping at all.[41]
Changes in eating frequently occur. Cognitive awareness is needed for eating and swallowing and progressive cognitive decline results in eating and swallowing difficulties. This can cause food to be refused, or choked on, and help with feeding will often be required.[45] For ease of feeding, food may be liquidized into a thick purée.[46] In some cases, terminal lucidity, a form of paradoxical lucidity, occurs immediately before death; in this phenomenon, there is an unexpected recovery of mental clarity.[47]
Types
Most types of dementia including Alzheimer's (the most common), Lewy body dementias, and frontotemporal dementia are neurodegenerative diseases, and protein misfolding is a cardinal feature of these.[48] The next most common type of dementia after Alzheimer's is vascular dementia, a cerebrovascular disease. These are the main primary types.[49] Secondary types of dementia are secondary to a pre-existing condition, such as Huntington's dementia secondary to Huntington's disease, and HIV-associated dementia secondary to HIV. Different dementias have different causes and risk factors.[14] But all types are characterized by loss of neurons, and consequent functioning.[8]Depressive cognitive disorder, formerly pseudodementia, describes dementia-like symptoms as a dementia secondary to a psychiatric condition especially to clinical depression.[50]
Alzheimer's disease, also called Alzheimer's dementia, accounts for 60–70% of cases of dementia worldwide. Alzheimer's is often part of a mixed dementia diagnosis, typically together with vascular dementia, but also with Lewy body dementia.[14] Mixed dementia has been acknowledged to be the most common type of dementia.[51]
Symptoms may vary among individuals. Typically one of the first signs is a problem with memory. Other cognitive impairments can include difficulty in finding the right word, difficulties with visuospatial ability, and impaired reasoning and judgment. In later stages the symptoms become more severe, and include greater confusion, and changes in behavior.[52]
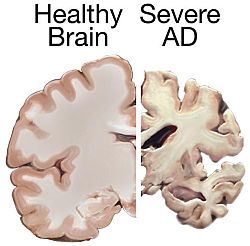
A lack of insight into having a condition will become evident.[42] The part of the brain most affected by Alzheimer's is the hippocampus in the medial temporal lobe. Other parts that show atrophy (shrinking) include the temporal and parietal lobes. Although this pattern of brain shrinkage suggests Alzheimer's, it is variable and at early stages a brain scan is insufficient for a diagnosis.[citation needed]
Historically, only brain tissue at autopsy could definitively diagnose Alzheimer's. CSF analysis has been available for detecting AD biomarkers. But blood-based biomarkers have taken the lead.[15]Flotillin has been proposed as a potential fluid biomarker for detecting early Alzheimers in either CSF or blood.[53] And a finger-prick blood sample for the diagnosis of early AD has been developed using p-tau 217 as biomarker.[54]
The hallmark features of Alzheimer's disease are the deposits of amyloid beta in extracellular amyloid plaques, and the intracellular neurofibrillary tangles formed by hyperphosphorylatedtau proteins.[56] Amyloid causes inflammation around the plaques, and excessive inflammation leads to irreversible changes in the brain that lead to the symptoms of Alzheimer's.[57] Amyloid PET imaging has made possible the development of anti-amyloid immunotherapies, such as donanemab, and lecanemab, for use in mild NCI due to Alzheimer's or in mild Alzheimer's.[51] For detecting tau protein another PET scan tracer flortaucipir was approved for use in the US and Europe in 2024.[58]
Kynurenine is a metabolite of tryptophan that regulates microbiome signaling, immune cell response, and neuronal excitation. A disruption in the kynurenine pathway may be associated with the neuropsychiatric symptoms and cognitive prognosis in mild AD dementia; lower numbers of kynurenines are found in those with Alzheimer's.[37]
Vascular dementia accounts for at least 20% of dementia cases, making it the second most common type.[59] It is caused by disease or injury affecting the blood supply to the brain, typically involving a series of mini-strokes. Symptoms depend on where in the brain the strokes occurred and whether the blood vessels affected were large or small.[41] Repeated injury can cause progressive dementia over time, while a single injury located in an area critical for cognition such as the hippocampus, or thalamus, can lead to sudden cognitive decline.[59] Elements of vascular dementia may be present in all other forms of dementia.[60]
The prodromal symptoms of dementia with Lewy bodies (DLB) include mild cognitive impairment, and delirium onset.[63] The symptoms of DLB are more frequent, more severe, and earlier presenting than in the other subtypes.[64] Dementia with Lewy bodies has the primary symptoms of fluctuating cognition, alertness or attention; REM sleep behavior disorder (RBD); one or more of the main features of parkinsonism, not due to medication or stroke; and repeated visual hallucinations.[65] The visual hallucinations in DLB are generally vivid hallucinations of people or animals and they often occur when someone is about to fall asleep or wake up. Other prominent symptoms include problems with planning (executive dysfunction) and difficulty with visual-spatial function,[41] and disruption in autonomic bodily functions.[66] Abnormal sleep behaviors may begin before cognitive decline is observed and are a core feature of DLB.[65] RBD is diagnosed either by sleep study recording or, when sleep studies cannot be performed, by medical history and validated questionnaires.[65]
Frontotemporal dementias (FTDs) are characterized by drastic personality changes, and language difficulties. In all types, early social withdrawal and lack of insight are major features but not memory problems.[67] The most common variant known as behavioral variant FTD (bv-FTD) presents major symptoms of changes in personality and behavior. The hallmark features of bv-FTD are impulsive behavior, and a lack of insight into having a condition, and these can be detected in pre-dementia states.[42][68] In bv-FTD, the person shows a change in personal hygiene, becomes rigid in their thinking, and rarely acknowledges problems; they are socially withdrawn, and often have a drastic increase in appetite. They may become socially inappropriate. For example, they may make inappropriate sexual comments, or may begin using pornography openly. One of the most common signs is apathy, or not caring about anything. Apathy, however, is a common symptom in many dementias.[41]
Other rare subtypes of FTD are three variants of primary progressive aphasia – language-led dementias that feature aphasia (language problems) as the main symptom.[12] One type is semantic dementia (or semantic PPA) with the main feature of the loss of the meaning of words.[69] Another type is called progressive nonfluent aphasia (or agrammatic PPA), mainly a difficulty in producing speech, not being able to find the right words, and also problems in coordinating the muscles needed for speech. Eventually the ability to talk at all may be lost.[69] The third type is logopenic progressive aphasia (discovered in 2004) and features impairment in the repetition of words or phrases, and impairment in retrieving words.[70]
More than one type of dementia, known as mixed dementia, may exist together in at least 10% of dementia cases. The most common type of mixed dementia is Alzheimer's disease and vascular dementia, and the second most common is Alzheimer's and Lewy body dementia. Mixed dementia occurs more frequently in the elderly and seem to progress more rapidly.[14] In 2025 an NIH study reported that mixed dementia has been acknowledged as the most common type of dementia.[51]
Diagnosis of mixed dementia can be difficult, as often only one type will predominate, which means that many people may miss out on potentially helpful treatments. Mixed dementia can mean that symptoms onset earlier, and worsen more quickly since more parts of the brain will be affected.[14]
Autoimmune dementia
Cognitive decline due to an autoimmune disease can be mistaken for that of a dementia subtype. The importance of correctly identifying an autoimmune dementia is critical in approved treatments. Being treated for dementia rules out immmunotherapy which could treat and reverse the disorder. Also to treat Alzheimer's with monoclonal antibodies would be contraindicated if there are unreported autoantibodies present.[71][72]
Around 7% of people over the age of 65 have dementia, with slightly higher rates (up to 10% of those over 65) in places with relatively high life expectancy.[74] Dementia can develop before the age of 65 when it is known as early onset dementia or young-onset dementia.[75]
A type of dementia has been classified as limbic-predominant age-related TDP-43 encephalopathy (LATE). It can only be diagnosed on autopsy when clusters of TDP-43 are found in the brain. It usually has a late onset typically affecting those over 80, and can also be found alongside Alzheimer's disease. [77]
Huntington's disease is a neurodegenerative disease caused by mutations in a single gene HTT, that encodes for huntingtin protein. Symptoms include cognitive impairment that usually declines further into dementia. Other symptoms include chorea (jerky movements), memory lapses, depression, stumbling and clumsiness, mood swings, and behavior changes such as impulsivity and irritability that can become more aggressive in later stages.[79]
HIV-associated dementia results as a late stage from HIV infection, and mostly affects younger people.[80] The essential features of HIV-associated dementia are disabling cognitive impairment accompanied by motor dysfunction, speech problems and behavioral change.[80] Cognitive impairment is characterised by mental slowness, trouble with memory and poor concentration. Motor symptoms include a loss of fine motor control leading to clumsiness, poor balance and tremors. Behavioral changes may include apathy, lethargy and diminished emotional responses and spontaneity. Histopathologically, it is identified by the infiltration of monocytes and macrophages into the central nervous system (CNS), gliosis, pallor of myelin sheaths, abnormalities of dendritic processes and neuronal loss.[81]
Alcohol-related dementia, occurs as a result of alcohol-related brain damage due to alcoholism. Different factors can be involved in this development including thiamine deficiency and age vulnerability. A degree of brain damage is seen in more than 70% of cases of alcoholism. Brain regions affected are similar to those that are affected by aging, and also by Alzheimer's. Regions showing loss of volume include the frontal, temporal, and parietal lobes, as well as the cerebellum, thalamus, and hippocampus. This loss can be more notable, with greater cognitive impairments seen in those aged 65 years and over.[83]
Conditions with dementia-like symptoms
Autoimmune dementias of autoimmune disorder origin can mimic subtypes of dementia. They are potentially treatable if recognized and can have a good response to immunotherapy.[72]
Celiac disease may increase the risk of vascular dementia. Gluten-related disorders might raise the risk of cognitive impairment which can be an early sign of dementia. A strict gluten-free diet started early may protect against this risk of vascular dementia.[84]
The symptoms of dementia may vary depending on the underlying subtype, and between individuals, particularly in the early stages but at the end stage of all types they are similar. Diagnosis by symptoms alone is difficult, made more so when there is more than one type.[49] A medical history will be taken, and cognitive testing carried out.[87]Blood tests can rule out possible treatable causes such as vitamin deficiencies and hormone imbalances, or rule in probable Alzheimer's. One or more types of scan may also be needed.[55] The DSM5 (2013) published by the American Psychiatric Association gives the diagnostic criteria for a primary dementia as the recognition of a significant decline in one or more cognitive domains that interfere with the ability to carry out everyday activities; the cognitive deficits are not exclusive to delirium, and are not explained by mental disorders such as schizophrenia, and major depressive disorder.[21][11]
A number of brief cognitive tests (5–15 minutes) are available that are reasonably reliable but results need to take into account the influence of a person's educational level.[87] The mini–mental state examination (MMSE) is the best studied and most commonly used test.[28] This is useful in diagnosis if the results are interpreted along with an assessment of a person's personality, their ability to perform activities of daily living, and their behavior.[4] Other cognitive tests include the abbreviated mental test score (AMTS), the modified mini–mental state examination (3MS),[88] the Cognitive Abilities Screening Instrument (CASI),[89] the Trail-making test,[90] and the clock drawing test.[91]The Montreal Cognitive Assessment (MoCA) is a reliable screening test and is freely available online in many languages.[92] The MoCA has also been shown to be somewhat better at detecting mild cognitive impairment than the MMSE.[30] An adapted version is available, suitable for those with hearing loss, that avoids the need for people to listen and respond to questions.[93] RUDAS, the Rowland Universal Dementia Assessment Scale, is a short dementia screening test for use in diverse multi-ethnic communities designed to overcome language and cultural differences.[94] An integrated cognitive assessment (CognICA) is a five-minute test that is highly sensitive to the early stages of dementia, and uses an application deliverable to an iPad.[95][96] Previously in use in the UK, in 2021 CognICA was given FDA approval for its commercial use as a medical device.[96]
Informant-based questionnaires are also widely used to gain a better understanding of the types and severity of cognitive decline, and also of behavioral changes. Possibly the best known is the Informant Questionnaire on Cognitive Decline in the Elderly.[97] A well-established one used to capture behavioral changes is the Neuropsychiatric Inventory (NPI).[98] A similar scale based on the NPI is the Cambridge Behavioural Inventory which has been shown to be able to differentiate the neurodegenerative disorders by grouping common behavioral symptoms.[99] The General Practitioner Assessment Of Cognition combines a patient assessment with an informant interview, designed for use in the primary care setting. The AD-8, an informant assessment for dementia screening questionnaire using eight items, is used to assess changes in function related to cognitive decline and is potentially useful, but is not diagnostic, is variable, and has risk of bias.[100]
Neuroimaging techniques are commonly used to rule out reversible causes of dementia such as normal pressure hydrocephalus. Scans can also show if the cause is a tumor, or show evidence of a stroke which would indicate vascular dementia.[55]PET-CT scans (functioning and structural, respectively) are useful in differentiating types of dementia.[55] A PET scan that uses a radiotracer, commonly FDG can highlight areas of low glucose metabolism in the brain. A pattern of reduced glucose metabolism shown in the temporal and parietal lobes is indicative of Alzheimer's, other patterns are particular to FTD or to LBD.[55]Amyloid imaging (amyloid PET) uses a radiotracer that binds to amyloid plaques (large numbers are a hallmark feature of Alzheimer's) to provide detailed images of the distribution of amyloid. This can show up years, even decades, before the onset of symptoms. Serial amyloid imaging shows amyloid beta deposits firstly in the anterior temporal areas that then spread to the frontal and medial parietal regions, the associative neocortex, and then to the primary sensorimotor areas and subcortical regions.[55][104]
Many of the risk factors are potentially modifiable. They include some that may be only partially causal but if they were all addressed nearly a half of dementia cases could be prevented. And a decreased risk is also possible for those with a genetic risk.[3] The two most modifiable risk factors for dementia are physical inactivity and lack of cognitive stimulation.[111]Physical activity, in particular aerobic exercise, is associated with a reduction in age-related brain tissue loss, and neurotoxic factors. Cognitive activity strengthens neural plasticity and together they help to support cognitive reserve.[111]
Impaired vision and hearing are modifiable risk factors.[112][113] These impairments may precede cognitive symptoms by many years.[114] Hearing loss may lead to another risk factor of social isolation which negatively affects cognition.[115][114] Age-related hearing loss is characterised by slowed central processing of auditory information.[114] Worldwide, mid-life hearing loss may account for around 9% of dementia cases.[115] Hearing loss is not a recognised risk factor for vascular dementia.[113]
Sarcopenia (age-related muscle loss) and resulting frailty may increase the risk of cognitive decline, and dementia, and the inverse also holds of cognitive impairment increasing the risk of frailty. Prevention of frailty may help to prevent cognitive decline.[116]
Other health conditions as comorbidities may be present; some such as high blood pressure or diabetes, are associated with a risk for dementia, and others such as depression, and anxiety are associated with dementia itself.[117]
There are no medications available that can prevent cognitive decline and dementia.[118] An economic model has proposed that population-level interventions in England that target dementia risk factors such as high blood pressure, smoking and obesity, could save money and give people extra years in good health. For example, reduced salt in food, to address hypertension, could give 39,433 quality-adjusted life-years and save £2.4 billion.[119]
The Mediterranean and DASH diets are both associated with less cognitive decline. A different approach has been to incorporate elements of both of these diets into one known as the MIND diet.[121] These diets are generally low in saturated fats while providing a good source of carbohydrates, mainly those that help stabilize blood sugar and insulin levels.[122] Raised blood sugar levels over a long time, can damage nerves and cause memory problems if they are not managed.[123] Nutritional factors associated with the proposed diets for reducing dementia risk include unsaturated fatty acids, vitamin E, vitamin C, flavonoids, vitamin B, and vitamin D.[124][125] A study conducted at the University of Exeter in the United Kingdom seems to have confirmed these findings with fruits, vegetables, whole grains, and healthy fats creating an optimum diet that can help reduce the risk of dementia by roughly 25%.[126]
The MIND diet may be more protective but further studies are needed. The Mediterranean diet seems to be more protective against Alzheimer's than DASH but there are no consistent findings against dementia in general.[121] The role of olive oil needs further study as it may be one of the most important components in reducing the risk of cognitive decline and dementia.[127]
Omega-3 fatty acid supplements do not appear to benefit or harm people with mild to moderate symptoms, but there is good evidence that they help in treating the common symptom of depression, and a potential risk factor for dementia.[129][3]
Dental health
Poor oral health has not been identified as a known risk factor for dementia but there is evidence for its association with cognitive decline. Different factors have been proposed including tooth infections that may have an inflammatory effect, and tooth loss that impairs proper chewing of food, impacting diet and quality of life.[130] Oral health declines with advancing cognitive impairment, due in part to an increased inability to maintain daily self-care, and also barriers to dental care access. Increasing evidence indicates that poor oral health may be more than just a result of dementia and could be a causative factor.[131][132]
There are several non-pharmacological, and limited pharmacological options for treating dementia, and no available options to delay the onset or stop the progression. Some types of medication are used to address the symptoms in different subtypes but the benefit is small.[133]
More than half of people with dementia may experience psychological or behavioral symptoms including agitation, sleep problems, aggression, and/or psychosis. Treatment for these symptoms is aimed at reducing the person's distress and keeping the person safe. Treatments other than medication appear to be better for agitation and aggression.[134] Cognitive and behavioral interventions may be appropriate. Exercise programs are beneficial with respect to activities of daily living.[135] As with all brain disorders, some people with dementia could potentially be a danger to themselves or others. Such behavioral symptoms might result in the person being involuntarily admitted to a mental health ward for assessment, care and treatment. However, this is a last resort, and potential alternatives could be considered by family or friends of people with dementia.[136][137]
Palliative care interventions may lead to improvements in the quality of life, management of symptoms, and comfort in dying, but it is not yet known how it can be best used to support people dying with advanced dementia and their families.[138]
Non-pharmacological interventions to address the behavioral and psychiatric symptoms of dementia include Montessori-based programmes.[139] Indicators for depression may use a Cornell Scale for Depression in Dementia (CSDD)[140][141]
Often overlooked in treating and managing dementia is the role of the caregiver and what is known about how they can support multiple interventions. Caregivers of people with dementia in nursing homes do not have sufficient tools or clinical guidance for behavioral and psychological symptoms of dementia (BPSD) along with medication use.[142] Simple measures like talking to people about their interests can improve the quality of life for care home residents living with dementia. A programme showed that such simple measures reduced residents' agitation and depression. They also needed fewer GP visits and hospital admissions, which also meant that the programme was cost-saving.[143][144]
Psychological therapies for dementia include some limited evidence for reminiscence therapy (namely, some positive effects in the areas of quality of life, cognition, communication and mood – the first three particularly in care home settings),[145] some benefit for cognitive reframing for caretakers,[146] unclear evidence for validation therapy[147] and tentative evidence for mental exercises, such as cognitive stimulation programs for people with mild to moderate dementia.[148] Offering personally tailored activities may help reduce challenging behavior and may improve quality of life.[149]
Adult daycare centers as well as special care units in nursing homes often provide specialized care for dementia patients. Daycare centers offer supervision, recreation, meals, and limited health care to participants, as well as providing respite for caregivers. In addition, home care can provide one-to-one support and care in the home allowing for more individualized attention that is needed as the disorder progresses. Psychiatric nurses can make a distinctive contribution to people's mental health.[150]
Dementia impairs normal communication and agitated behavior is often used to indicate pain, illness, or overstimulation.[151] The strongest evidence for non-pharmacological therapies for the management of changed behaviors in dementia is for using such approaches.[152] Low quality evidence suggests that regular (at least five sessions of) music therapy may help institutionalized residents. It may reduce depressive symptoms and improve overall behaviors. It may also supply a beneficial effect on emotional well-being and quality of life, as well as reduce anxiety.[153] In 2003, The Alzheimer's Society established 'Singing for the Brain' (SftB) a project based on pilot studies which suggested that the activity encouraged participation and facilitated the learning of new songs. The sessions combine aspects of reminiscence therapy and music.[154] Musical and interpersonal connectedness can underscore the value of the person and improve quality of life.[155]
Some London hospitals found that using color, designs, pictures and lights helped people with dementia adjust to being at the hospital. These adjustments to the layout of the dementia wings at these hospitals helped patients by preventing confusion.[156]
Life story work as part of reminiscence therapy, and video biographies have been found to address the needs of clients and their caregivers in various ways, offering the client the opportunity to leave a legacy and enhance their personhood and also benefitting youth who participate in such work. Such interventions can be more beneficial when undertaken at a relatively early stage of dementia. They may also be problematic in those who have difficulties in processing past experiences[155]
Occupational therapy also addresses psychological and psychosocial needs of patients with dementia through improving daily occupational performance and caregivers' competence.[157] When compensatory intervention strategies are added to their daily routine, the level of performance is enhanced and reduces the burden commonly placed on their caregivers.[157] Occupational therapists can also work with other disciplines to create a client centered intervention.[158] To manage cognitive disability, and coping with behavioral and psychological symptoms of dementia, combined occupational and behavioral therapies can support patients with dementia even further.[158]
Cognitive training and rehabilitation
There is no strong evidence to suggest that cognitive training is beneficial for people with Parkinson's disease, dementia, or mild cognitive impairment.[159] However, a 2023 review found that cognitive rehabilitation may be effective in helping individuals with mild to moderate dementia to manage their daily activities.[160]
Medications
Donepezil
There are some medications used in the treatment of symptoms of the different dementias. Acetylcholinesterase inhibitors, such as donepezil, may be useful for Alzheimer's disease.[161] Moderate-quality evidence shows that donepezil provides small improvements in cognition, daily functioning, and global clinical state in Alzheimer's disease, with higher doses slightly increasing benefit but also adverse events.[162] No difference has been shown between the agents in this family.[163] In a minority of people side effects include a slow heart rate and fainting.[164]Rivastigmine is recommended for treating symptoms in Parkinson's disease dementia.[6]
Medications that have anticholinergic effects increase all-cause mortality in people with dementia, although the effect of these medications on cognitive function remains uncertain, according to a systematic review published in 2021.[165]
Before prescribing antipsychotic medication in the elderly, an assessment for an underlying cause of the behavior is needed.[166] Severe and life-threatening reactions occur in almost half of people with DLB,[66][167] and can be fatal after a single dose.[168] People with Lewy body dementias who take neuroleptics are at risk for neuroleptic malignant syndrome, a life-threatening illness.[169] Extreme caution is required in the use of antipsychotic medication in people with DLB because of their sensitivity to these agents.[65] Antipsychotic drugs are used to treat dementia only if non-drug therapies have not worked, and the person's actions threaten themselves or others.[170][171] Aggressive behavior changes are sometimes the result of other solvable problems, that could make treatment with antipsychotics unnecessary.[166] Because people with dementia can be aggressive, resistant to their treatment, and otherwise disruptive, sometimes antipsychotic drugs are considered as a therapy in response.[166] These drugs have risky adverse effects, including increasing the person's chance of stroke and death.[166] Given these adverse events and small benefit antipsychotics are avoided whenever possible.[152] Generally, stopping antipsychotics for people with dementia does not cause problems, even in those who have been on them a long time.[172]
Memantine provides a small but consistent benefit for moderate-to-severe Alzheimer's disease, regardless of cholinesterase inhibitor use, but shows no clear benefit and may increase adverse events in mild Alzheimer's, with limited evidence for other dementias.[173] Due to their differing mechanisms of action memantine and acetylcholinesterase inhibitors can be used in combination however the benefit is slight.[174][175]
An extract of Ginkgo biloba known as EGb 761 has been widely used for treating mild to moderate dementia and other neuropsychiatric disorders.[176] Its use is approved throughout Europe.[177] The World Federation of Biological Psychiatry guidelines lists EGb 761 with the same weight of evidence (level B) given to acetylcholinesterase inhibitors, and memantine. EGb 761 is the only one that showed improvement of symptoms in both AD and vascular dementia. EGb 761 is seen as being able to play an important role either on its own or as an add-on particularly when other therapies prove ineffective.[176] EGb 761 is seen to be neuroprotective; it is a free radical scavenger, improves mitochondrial function, and modulates serotonin and dopamine levels. Many studies of its use in mild to moderate dementia have shown it to significantly improve cognitive function, activities of daily living, neuropsychiatric symptoms, and quality of life.[176][178] However, its use has not been shown to prevent the progression of dementia.[176]
No evidence supports the use of vitamin or mineral supplements including B vitamins to improve cognitive impairment.[182] No evidence supports the use of statins to prevent dementia.[183] Medications for other health conditions may need to be managed differently for a person who has a dementia diagnosis. It is unclear whether blood pressure medication and dementia are linked. People may experience an increase in cardiovascular-related events if these medications are withdrawn.[184]
The Medication Appropriateness Tool for Comorbid Health Conditions in Dementia (MATCH-D) criteria can help identify ways that a diagnosis of dementia changes medication management for comorbidities (other health conditions).[185] These criteria were developed because people with dementia live with an average of five other chronic diseases, which are often managed with medications. The systematic review that informed the criteria were published subsequently in 2018 and updated in 2022.[186]
Palliative care
Palliative care, the total care given by a team of health care providers can be helpful to both the individual and the caregiver.[34] It aims to improve quality of life, at all stages.[187] It can help people with dementia and their caregivers to understand what to expect, deal with loss of physical and mental abilities, support the person's wishes and goals including surrogate decision making, and discuss wishes for or against CPR and life support.[188]
Because there is uncertainty around how and when people with dementia decline, and because most people prefer to allow the person with dementia to make their own decisions, palliative care involvement before the late stages of dementia is recommended.[189] In the early stages of dementia, palliative care can involve advocacy around establishing goals of care in the future, reassurance of continued support, planning for future scenarios of care and establishing long-term relationships with care providers.[190] In later stages, a palliative approach to dementia care may have specific benefit to goals of care and end-of-life conversations, symptom management, prescribing practices and emergency department visits.[191] More research is needed to know how palliative care can be best used to support people at end-of-life needs.[34] dying with advanced dementia and their families.[192]
Towards the end of life, without palliative care, people often present to the emergency department.[193] Community palliative care is associated without this need.[194]End-of-life care outcomes at home, such as neuropsychiatric symptoms may be improved.[195]
People with advanced dementia may not readily receive specialist palliative care input.[196] Reasons for this are varied but may include lack of agreement of when to refer people with dementia,[197] and a lack of coordination across care settings, communication challenges, limited training opportunities for healthcare staff and because dementia is considered to be a life-limiting condition.[196] Dementia is often thought to be a normal ageing process and not recognized as a terminal condition.[19][198] Further research is needed to determine the appropriate palliative care interventions and how they can be implemented.[138][195]
Person-centered care
Person-centered care (different from patient participation), takes into account the individual's needs, preferences, experiences, and values. It is built on getting to know the person with the condition through a personal relationship.[199] This is especially important as the approach aims to maintain the dignity of people with dementia and sense of identity throughout the course of their illness.[200]
Person-centered care interventions could not only reduce agitation, neuropsychiatric symptoms, and depression but also help improve the quality of life for people with dementia.[201] Moreover, the potential benefits of a person-centered care approach for dementia care workers have been reported, indicating its effectiveness in reducing stress, burnout, and job dissatisfaction.[199][202]Person-centered outcome measures (PCOMs) are standardized, validated questionnaires that measure people's opinions of their own health and well-being. They emphasize person-centered care by focusing on the symptoms and concerns that are most important to people and their families.[203][204] PCOMs may be self-reported (when the person with dementia completes the questionnaire) or proxy-reported (when the questionnaire is completed by someone who knows them well). Proxy-reported PCOMs are used in more advanced stages of dementia when the person is no longer able to self report.[203] Used in routine care, PCOMs support systematic assessment and monitoring of an individual's health and wellbeing, enable shared decision-making, enable changes in care provision (such as improved communication or referral to other services), improve outcomes (such as improved symptom management) and enable evaluation of care provision.[203] The use of PCOMs have the potential to serve as a scalable and sustainable way to support integrated palliative care for older people including those living with dementia.[204]
PCOMs can be single-domain or multi-domain tools, focussing on individual symptoms or multiple symptoms.[205] Single-domain PCOMs focus on one specific area of care such as the Pain Assessment in Advanced Dementia scale,[206] Multi-domain PCOMs can assess symptom burden, function, psychological, and spiritual concerns for example. The Integrated Palliative Care Outcome Scale for Dementia is a comprehensive palliative dementia PCOM, used to measure symptoms and concerns for people with dementia and their family.[207]
Sleep disturbances
Over 40% of people with dementia report sleep problems.[208] Approaches to treating these sleep problems include medications and non-pharmacological approaches.[208] The use of medications to alleviate sleep disturbances has not been well researched, even for medications that are commonly prescribed.[209] In 2012 the American Geriatrics Society recommended that benzodiazepines such as diazepam, and non-benzodiazepine sleeping pills, be avoided for people with dementia due to the risks of increased cognitive impairment and falls.[210] Benzodiazepines are also known to promote delirium.[211] Additionally, little evidence supports the effectiveness of benzodiazepines in this population.[209][212] No clear evidence shows that melatonin or ramelteon improves sleep for people with dementia due to Alzheimer's,[209] but it is used to treat REM sleep behavior disorder in dementia with Lewy bodies.[66] Limited evidence suggests that a low dose of trazodone may improve sleep, however more research is needed.[209]
Non-pharmacological approaches have been suggested but there is no strong evidence or firm conclusions on the effectiveness of different types of interventions, especially for those who are living in an institutionalized setting such as a nursing home or long-term care home.[208] A sleep management programme may be useful that includes sleep hygiene education, exercise and tailored activities.[170]
Pain in those with dementia is often overlooked and poorly assessed since they become incapable of communicating their pain.[213][214] Persistent pain has functional implications, it can lead to decreased ambulation, depression, sleep disturbances, impaired appetite, and exacerbation of cognitive impairment[214] and be a factor contributing to falls in the elderly.[213][215] Nearly 80% of those with dementia in nursing homes may experience pain that is difficult to assess as communication is difficult, and it may be expressed as a behavioral symptom.[216][217]
Family members and friends can learn to recognize and assess their pain. Educational resources and observational assessment tools are available.[213][218]
Eating difficulties
Persons with dementia may have difficulty eating. Whenever it is available as an option, the recommended response to eating problems is having a caretaker assist them.[166] For people who do not have dementia, a secondary option when they cannot swallow effectively would be to consider gastrostomyfeeding tube placement as a way to give nutrition. However, for people with dementia, assistance with oral feeding is at least as good as tube feeding in bringing comfort and maintaining functional status while lowering risk of aspiration pneumonia and death[166] It can be tried if the reasons for the person's problems with eating, drinking or swallowing are treatable and it's expected that they will be able to start eating and drinking normally afterwards.[219] Tube-feeding is associated with agitation, increased use of physical and chemical restraints and worsening pressure ulcers. Tube feedings may cause fluid overload, diarrhea, abdominal pain, local complications, less human interaction and may increase the risk of aspiration.[166]
Benefits in those with advanced dementia has not been shown.[220] The risks of using tube feeding include agitation, rejection by the person (pulling out the tube, or otherwise physical or chemical immobilization to prevent them from doing this), or developing pressure ulcers.[166] The procedure is directly related to a 1% fatality rate[221] with a 3% major complication rate.[222] The percentage of people at end of life with dementia using feeding tubes in the US has dropped from 12% in 2000 to 6% as of 2014.[223][224]
The immediate and long-term effects of modifying the thickness of fluids for swallowing difficulties in people with dementia are not well known.[225] While thickening fluids may have an immediate positive effect on swallowing and improving oral intake, the long-term impact on the health of the person with dementia should also be considered.[225]
Exercise programs may improve the ability of people with dementia to perform daily activities, but the best type of exercise is still unclear.[226] Getting more exercise can slow the development of cognitive problems such as dementia, proving to reduce the risk of Alzheimer's disease by about 50%. A balance of strength exercise, to help muscles pump blood to the brain, and balance exercises are recommended for aging people. A suggested amount of about 2+1⁄2 hours per week can reduce risks of cognitive decay as well as other health risks like falling.[227]
Assistive technology and digital health
There is a lack of high-quality scientific evidence to determine whether assistive technology effectively supports people with dementia to manage memory issues.[228] Some of the specific things that are used today that helps with dementia today are: clocks, communication aids, electrical appliances the use monitoring, GPS location/ tracking devices, home care robots, in-home cameras, and medication management are just to name a few.[229] As the technology advances, virtual reality is also being explored as a powerful technology to elicit memories and to improve wellbeing.[230]
Technology has the potential to be a valuable intervention for alleviating loneliness and promoting social connections.[231] It could facilitate activities of daily living, and provide ways to connect people that are geographically distant.[232]
Other types of developed technologies to aid services include telehealth or telemedicine services, using digital communication for delivery of health-related services and information through phone calls, mobile apps, and video conferencing.[233]
Telemedicine has given results for cognitive assessment and diagnosis that are similar to in-person visits, and it has also helped improve outcomes after rehabilitation. Telemedicine is often well received by people affected by dementia who can rely on the support of staff and family to navigate the technology. While it has potential to widen access to services, those with sensory impairment may be excluded.[233]
Digital health interventions can play a role in supporting family caregivers of people with dementia, by offering a source of support from connective platforms, with 24/7 accessibility, as well as opportunity for remote monitoring. However, challenges such as the digital divide, privacy concerns and the need for greater personalisation for individual users are recognised issues.[233]
Remotely delivered interventions including support, training and information may reduce the burden for the informal caregiver and improve their depressive symptoms.[234] There is no certain evidence that they improve health-related quality of life.[234]
In several localities in Japan, digital surveillance may be made available to family members, if a person with dementia is prone to wandering and going missing.[235]
Suicide risk following diagnosis
Individuals diagnosed with dementia, particularly in the early stages, may face an elevated risk of suicide. The risk of suicide is significantly higher within the first three months and up until to a year after a dementia diagnosis, especially among patients diagnosed before the age of 65.[236]
Alternative medicine
Scientific evidence of the therapeutic values of aromatherapy and massage is unclear and limited. There is no convincing evidence about their effectiveness but no general conclusions can be drawn about the benefits or harms of these alternative treatments.[237][238] It is not clear if cannabidiol has any harmful or beneficial effects on dementia.[239]
The number of cases of dementia worldwide in 2021 was estimated at 57 million, with close to 10million new cases each year.[1] It is (as of 2026) the seventh leading cause of death with some 1.8 million lost lives in 2021.[1][240] By 2050, the number of people living with dementia around the world is estimated to be over 150million.[241] Globally, the fastest increase in serious health-related suffering by 2060 is expected to occur among people with dementia.[242]
Around 7% of people over the age of 65 have dementia, with slightly higher rates, up to 10%, in places with relatively high life expectancy.[74] An estimated 58% of people with dementia are living in low and middle income countries.[243]
The prevalence of dementia differs in different world regions, ranging from 4.7% in Central Europe to 8.7% in North Africa/Middle East; the prevalence in other regions is estimated to be between 5.6 and 7.6%.[243] The number of people living with dementia is estimated to double every 20 years.[243]
Estimates show that in 2024 there were 982,000 people living with dementia in the UK and this is expected to rise to 1.4 million people by 2040.[244]
The annual incidence of dementia diagnosis is nearly 10 million worldwide.[138] Almost half of new dementia cases occur in Asia, followed by Europe (25%), the Americas (18%) and Africa (8%). The incidence of dementia increases exponentially with age, doubling with every 6.3-year increase in age.[243] Dementia affects 5% of the population older than 65 and 20–40% of those older than 85.[245] Rates are slightly higher in women than men at ages 65 and greater.[245] The disease trajectory is varied and the median time from diagnosis to death depends strongly on age at diagnosis, from 6.7 years for people diagnosed aged 60–69 to 1.9 years for people diagnosed at 90 or older.[138]
In 2019, there were 1.62 million dementia-related deaths worldwide. This is expected to increase to 4.91 million by 2050.[7]
In 2022 and 2023, dementia was the leading cause of death in England and Wales.[17]
Deaths from dementia in the U.S. have tripled in the past 21 years, rising from around 150,000 in 1999 to over 450,000 in 2020, and the likelihood of dying from dementia increased across all demographic groups.[246]
The genetic and environmental risk factors for dementia disorders vary by ethnicity.[247][248] For instance, Alzheimer's disease among Hispanic/Latino and African American subjects exhibit lower risks associated with gene changes in the apolipoprotein E gene than do non-Hispanic white subjects.[249]
In the United States in 2017, over 37% of dementia cases were associated with cardiometabolic conditions, though the risk varies across regions. The eight key contributors were diabetes, heart failure, atrial fibrillation, coronary artery disease, heart attacks, strokes, hypertension and high cholesterol. Among these, stroke was the most significant factor, doubling the risk of developing dementia (2.2 times higher), followed closely by heart failure (2.1 times) and hypertension (78% increased risk). In contrast, high cholesterol had the weakest correlation, associated with a 27% increased risk. However, there were also geographic disparities, and individuals living in the U.S. South faced a higher likelihood of dementia related to cardiovascular conditions and diabetes.[250][251]
Inequities and inequalities
inequalities and inequities are observed in the risk of developing dementia, in the ability to take part in prevention efforts, and in access to high-quality care from diagnosis until the end of life, including bereavement support.[252]
Post-diagnostic care is often variable and difficult to navigate,[253][254][255] with a disparity in care between dementia and other life-limiting conditions.[256][257][258] Furthermore, substantially less dementia research funding and financial support for the care of people with dementia compared to other life-limiting conditions also exists.[252]
Differences in access to high-quality care among dementia subtypes are also noted. People with rare types of dementia compared to those with Alzheimer's Disease, and those with other physical conditions are less likely to experience high-quality care.[259]
People with dementia are often physically or chemically restrained to a greater degree than necessary, raising issues of human rights.[1]Social stigma is commonly perceived by those with the condition, and also by their caregivers.[1]
Socioeconomic status and deprivation
There are significant advantages associated with having a timely dementia diagnosis (i.e., receiving the diagnosis at the milder stages of the condition). However, access to dementia diagnosis can be inequitable. Compared to individuals with high socioeconomic status, those with low socioeconomic status can have more than three-times higher risk of early-onset dementia. Additionally, individuals of low socioeconomic status with unhealthy lifestyles, can have 440% greater risk of developing early-onset dementia compared with individuals of high socioeconomic status with healthy lifestyles.[3] Measures to improve social determinants of health are warranted, as healthy lifestyle promotion alone might not substantially reduce the socioeconomic inequity in early-onset dementia and late-onset dementia risk.
People with dementia residing in rural areas often experience challenges in receiving a timely diagnosis and accessing health and social care compared to people living in urban areas.[260]
Among older people diagnosed with dementia, those from most deprived areas can be more likely to experience hospitalisations, emergency department visits, potentially inappropriate medication prescriptions, and higher 1-year mortality.[261] People living in the most deprived areas are more likely to experience multiple hospitalisations in the last three months of life and emergency department visits in the last year of life.[262][263] In high-income countries, low socioeconomic position is a risk factor for dying in hospital as well as other indicators of potentially poor-quality end-of-life care.[264]
Race and ethnicity
Significant differences in dementia incidence and risk exist based on race and ethnicity. The mechanisms responsible for these differences are not yet understood.[265][266] People who are Black in the US are at risk of receiving more futile and invasive treatment towards the end of life.[267] Emerging evidence from other countries also suggest that minority groups from different cultures, ethnicities may experience sub-optimal care from diagnosis to the end-of-life.[268][262][269][270]
Gender
Globally, women are much more impacted by dementia than men. Two in three people with dementia are women. Yet, medical data from women are lacking compared to men. Women are more likely to care for another person with dementia (in the workforce and informally). The proportion of women caregivers in low and middle income countries is higher.[271][272]Gender disparities exist towards the end-of-life in palliative caregiving and end-of-life care experiences.[273]
Until the end of the 19th century, dementia was a much broader clinical concept. It included mental illness and any type of psychosocial incapacity, including reversible conditions.[274]Dementia at this time simply referred to anyone who had lost the ability to reason, and was applied equally to psychosis, organic diseases like syphilis that destroy the brain, and to the dementia associated with old age, which was attributed to "hardening of the arteries".[citation needed]
A 19th-century drawing of a woman diagnosed with dementia
Dementia has been referred to in medical texts since antiquity. One of the earliest known allusions to dementia is attributed to the 7th-century BC Greek philosopherPythagoras, who divided the human lifespan into six distinct phases: 0–6 (infancy), 7–21 (adolescence), 22–49 (young adulthood), 50–62 (middle age), 63–79 (old age), and 80–death (advanced age). The last two he described as the "senium", a period of mental and physical decay, and that the final phase was when "the scene of mortal existence closes after a great length of time that very fortunately, few of the human species arrive at, where the mind is reduced to the imbecility of the first epoch of infancy".[275] In 550BC, the Athenian statesman and poet Solon argued that the terms of a man's will might be invalidated if he exhibited loss of judgement due to advanced age. Chinese medical texts made allusions to the condition as well, and the characters for "dementia" translate literally to "foolish old person".[276]
Athenian philosophers Aristotle and Plato discussed the mental decline that can come with old age and predicted that this affects everyone who becomes old and nothing can be done to stop this decline from taking place. Plato specifically talked about how the elderly should not be in positions that require responsibility because, "There is not much acumen of the mind that once carried them in their youth, those characteristics one would call judgement, imagination, power of reasoning, and memory. They see them gradually blunted by deterioration and can hardly fulfill their function."[277]
For comparison, the Roman statesman Cicero held a view much more in line with modern-day medical wisdom that loss of mental function was not inevitable in the elderly and "affected only those old men who were weak-willed". He spoke of how those who remained mentally active and eager to learn new things could stave off dementia. However, Cicero's views on aging, although progressive, were largely ignored in a world that would be dominated for centuries by Aristotle's medical writings. Physicians during the Roman Empire, such as Galen and Celsus, simply repeated the beliefs of Aristotle while adding few new contributions to medical knowledge.
Byzantine physicians sometimes wrote of dementia. It is recorded that at least seven emperors whose lifespans exceeded 70 years displayed signs of cognitive decline. In Constantinople, special hospitals housed those diagnosed with dementia or insanity, but these did not apply to the emperors, who were above the law and whose health conditions could not be publicly acknowledged.
Poets, playwrights, and other writers made frequent allusions to the loss of mental function in old age. William Shakespeare notably mentions it in the plays Hamlet and King Lear.
During the 19th century, doctors generally came to believe that elderly dementia was the result of cerebral atherosclerosis, although opinions fluctuated between the idea that it was due to blockage of the major arteries supplying the brain or small strokes within the vessels of the cerebral cortex.
In 1907, Bavarian psychiatrist Alois Alzheimer was the first to identify and describe the characteristics of progressive dementia in the brain of 51-year-old Auguste Deter.[278] Deter had begun to behave uncharacteristically, including accusing her husband of adultery, neglecting household chores, exhibiting difficulties writing and engaging in conversations, heightened insomnia, and loss of directional sense.[279] At one point, Deter was reported to have "dragged a bed sheet outside, wandered around wildly, and cried for hours at midnight".[279] Alzheimer began treating Deter when she entered a Frankfurt mental hospital on November 25, 1901.[279] During her ongoing treatment, Deter and her husband struggled to afford the cost of the medical care, and Alzheimer agreed to continue her treatment in exchange for Deter's medical records and donation of her brain upon death.[279] Deter died on April 8, 1906, after succumbing to sepsis and pneumonia.[279] Alzheimer conducted the brain biopsy using the Bielschowsky stain method, which was a new development at the time, and he observed senile plaques, neurofibrillary tangles, and atherosclerotic alteration.[278] At the time, the consensus among medical doctors had been that senile plaques were generally found in older patients, and the occurrence of neurofibrillary tangles was an entirely new observation at the time.[279] Alzheimer presented his findings at the 37th psychiatry conference of southwestern Germany in Tübingen on April 11, 1906; however, the information was poorly received by his peers.[279] By 1910, Alois Alzheimer's teacher, Emil Kraepelin, published a book in which he coined the term "Alzheimer's disease" in an attempt to acknowledge the importance of Alzheimer's discovery.[278][279]
By the 1960s, the link between neurodegenerative diseases and age-related cognitive decline had become more established. By the 1970s, the medical community maintained that vascular dementia was rarer than previously thought and Alzheimer's disease caused the vast majority of old age mental impairments. More recently however, it is believed that dementia is often a mixture of conditions.
In 1976, neurologist Robert Katzmann suggested a link between senile dementia and Alzheimer's disease.[280] Katzmann suggested that much of the senile dementia occurring (by definition) after the age of 65, was pathologically identical with Alzheimer's disease occurring in people under age 65 and therefore should not be treated differently.[281] Katzmann thus suggested that Alzheimer's disease, if taken to occur over age 65, is actually common, not rare, and was the fourth- or 5th-leading cause of death, even though rarely reported on death certificates in 1976.
A helpful finding was that although the incidence of Alzheimer's disease increased with age (from 5–10% of 75-year-olds to as many as 40–50% of 90-year-olds), no threshold was found by which age all persons developed it. This is shown by documented supercentenarians (people living to 110 or more) who experienced no substantial cognitive impairment. Some evidence suggests that dementia is most likely to develop between ages 80 and 84 and individuals who pass that point without being affected have a lower chance of developing it.[citation needed] Women account for a larger percentage of dementia cases than men.[282] This can be attributed in part to their longer overall lifespan and greater odds of attaining an age where the condition is likely to occur.[283]
Much like other diseases associated with aging, dementia was comparatively rare before the 20th century, because few people lived past 80. Conversely, syphilitic dementia was widespread in the developed world until it was largely eradicated by the use of penicillin after World War II. With significant increases in life expectancy thereafter, the number of people over 65 started rapidly climbing. While elderly persons constituted an average of 3–5% of the population prior to 1945, by 2010 many countries reached 10–14% and in Germany and Japan, this figure exceeded 20%. Public awareness of Alzheimer's Disease greatly increased in 1994 when former US president Ronald Reagan announced that he had been diagnosed with the condition.
In the 21st century, other types of dementia were differentiated from Alzheimer's disease and vascular dementias (the most common types). This differentiation is on the basis of pathological examination of brain tissues, by symptomatology, and by different patterns of brain metabolic activity in nuclear medical imaging tests such as SPECT and PET scans of the brain. The various forms have differing prognoses and differing epidemiologic risk factors.
Terminology
Dementia derives from demens meaning out of mind.[284] In the elderly it was once called senile dementia or senility which are now outdated terms. The condition was viewed as a normal and somewhat inevitable aspect of aging.[285]
By 1913–20 the term dementia praecox was introduced to suggest the development of senile-type dementia at a younger age. Eventually the two terms fused, so that until 1952 physicians used the terms dementia praecox (precocious dementia) and schizophrenia interchangeably. Since then, science has determined that dementia and schizophrenia are two different disorders, though they share some similarities.[citation needed] The term precocious dementia for a mental illness suggested that a type of mental illness like schizophrenia (including paranoia and decreased cognitive capacity) could be expected to arrive normally in all persons with greater age (see paraphrenia). After about 1920, the beginning use of dementia for what is now understood as schizophrenia and senile dementia helped limit the word's meaning to "permanent, irreversible mental deterioration". This began the change to the later use of the term and researchers have seen a connection between those diagnosed with schizophrenia and patients who are diagnosed with dementia, finding a positive correlation between the two diseases.[286]
The view that dementia must always be the result of a particular disease process led for a time to the proposed diagnosis of "senile dementia of the Alzheimer's type" (SDAT) in persons over the age of 65, with "Alzheimer's disease" diagnosed in persons younger than 65 who had the same pathology. Eventually, however, it was agreed that the age limit was artificial, and that Alzheimer's disease was the appropriate term for persons with that particular brain pathology, regardless of age.[citation needed]
After 1952, mental illnesses including schizophrenia were removed from the category of organic brain syndromes, and thus (by definition) removed from possible causes of "dementing illnesses" (dementias). At the same, however, the traditional cause of senile dementia – "hardening of the arteries" – now returned as a set of dementias of vascular cause (small strokes). These were now termed multi-infarct dementias or vascular dementias.[citation needed]
Society and culture
Dementia impacts not only the individual, but also their carers and the wider society. Among people aged 60 years and over, dementia is ranked as the 9th most burdensome condition in the 2010 Global Burden of Disease Study estimates.[243]
The societal cost of dementia is high, especially for caregivers.[287] According to research conducted in the UK, almost two out of three carers of people with dementia feel lonely. Most of the carers in the study were family members or friends.[288][289]Family carers of people with dementia are at higher risk of developing psychological and physical conditions.[290]
National policies on dementia
The World Health Organization's (WHO) global action plan on the public health response to dementia (2017-2025) set a target for 75% of WHO Member States (194 countries) to develop a policy or plan for dementia by 2025. These plans recognize that people can live well with dementia for years, as long as the right support and timely access to a diagnosis are available. However, in 2025, only 23% of Member States (45 countries) have a national policy for dementia.[291]
Financial costs
The financial costs of care in people with dementia are high and tend to increase with end-of-life care. Long-term care facility and informal care costs are among the highest cost components, while non-White ethnicity, female sex, married status, higher education level, more severe dementia, and higher number of chronic conditions are associated with higher costs.[290]
The global costs of dementia was around US$818billion in 2015, a 35.4% increase from US$604billion in 2010.[243] By 2050 the estimated global cost will be $9.12trillion.[292]
In 2015, the annual cost per person with Alzheimer's in the United States was around $19,144.36.[290] The total costs for the country was estimated to be about $167.74billion. By 2030, it is predicted the annual socioeconomic cost will total to about $507billion, and by 2050 that number is expected to reach $1.89trillion.[292]
The total cost of dementia care in the UK is projected to increase by 172%, from £34.7 billion in 2019 to £94.1 billion in 2040.[290]
The estimated costs of dementia in low- and middle-income countries (LMICs) are lower compared to high-income countries, with indirect costs making up the largest proportion in LMICs. However, these estimates are likely an underrepresentation, as there have been limited research studies on dementia costs in LMICs, particularly low-income countries.[293][294]
Awareness
A worldwide study in 2019 showed that about 66% of the general public believe that dementia is a normal part of aging, and not a disorder, and 62% of healthcare professionals also held this view.[295] A follow-up study in 2024 showed that this figure had increased to 80% in the general public and to 65% among healthcare workers.[296] In 2022, only 42% of surveyed public in England knew that dementia is a terminal condition, and over 90% were unaware that dementia was the leading cause of cause of death in their country.[297] There is also persistent stigma, which can be a barrier for people seeking help for dementia and accessing care.[296][298] In 2024 88% of people living with dementia reported experiencing discrimination, an increase of 5% from 2019.[296] Over 64% of the general public believe people with dementia are impulsive and unpredictable.[296]
In October 2020, the Caretaker's (James Leyland Kirby) last music release, Everywhere at the End of Time, was popularized by TikTok users for its depiction of the stages of dementia. Kirby said that the use of the recordings could cause empathy among a younger public.[310]
On November 2, 2020, Scottish billionaire Tom Hunter donated £1million, split between Alzheimer's society, and Music for dementia. This donation was prompted after watching a former music teacher with dementia, Paul Harvey, playing one of his own compositions on the piano in a video.[311]
Research directions
Efforts to facilitate research into people living with dementia include the development of the Dementia Enquirers Gold Standards for Co-Research, and for Ethical Research.[312][313] Evidence-informed guidelines to involve people with impaired mental nearing the end of life have also been published.[314] And there are dedicated networks such as the UK-based EMPOWER Dementia Network+, which uses a co-productive approach to engage and include people from under-represented communities to tackle inequalities in dementia care and research.[315]
A 2026 Dementia Care and Caregiving Research Summit, hosted by the National Institute of Aging will review progress made in research, identify unmet research needs, and highlight research that is promising, and innovative.[316]
12Breton A, Casey D, Arnaoutoglou NA (February 2019). "Cognitive tests for the detection of mild cognitive impairment (MCI), the prodromal stage of dementia: Meta-analysis of diagnostic accuracy studies". International Journal of Geriatric Psychiatry. 34 (2): 233–242. doi:10.1002/gps.5016. PMID30370616. S2CID53097138.
↑Jurek L, Herrmann M, Bonze M, etal. (March 1, 2018). "Behavioral and psychological symptoms in Lewy body disease: a review". Gériatrie et Psychologie Neuropsychiatrie du Vieillissement. 16 (1): 87–95. doi:10.1684/pnv.2018.0723. PMID29569570.
↑Gray F, Adle-Biassette H, Chretien F, etal. (2001). "Neuropathology and neurodegeneration in human immunodeficiency virus infection. Pathogenesis of HIV-induced lesions of the brain, correlations with HIV-associated disorders and modifications according to treatments". Clinical Neuropathology. 20 (4): 146–155. PMID11495003.
↑Gleason OC (March 2003). "Delirium". American Family Physician. 67 (5): 1027–1034. PMID12643363. Archived from the original on September 29, 2007.
↑Caplan JP, Rabinowitz T (November 2010). "An approach to the patient with cognitive impairment: delirium and dementia". The Medical Clinics of North America. 94 (6): 1103–1116, ix. doi:10.1016/j.mcna.2010.08.004. PMID20951272.
↑Makhlouf S, Messelmani M, Zaouali J, etal. (2018). "Cognitive impairment in celiac disease and non-celiac gluten sensitivity: review of literature on the main cognitive impairments, the imaging and the effect of gluten free diet". Acta Neurol Belg (Review). 118 (1): 21–27. doi:10.1007/s13760-017-0870-z. PMID29247390. S2CID3943047.
↑Jeon YH, Li Z, Low LF, etal. (August 2015). "The clinical utility of the Cornell Scale for Depression in Dementia as a routine assessment in nursing homes". The American Journal of Geriatric Psychiatry. 23 (8): 784–793. doi:10.1016/j.jagp.2014.08.013. PMID25256214.
↑Harper AE, Rouch S, Leland NE, etal. (April 2022). "A Systematic Review of Tools Assessing the Perspective of Caregivers of Residents With Dementia". Journal of Applied Gerontology. 41 (4): 1196–1208. doi:10.1177/07334648211028692. PMID34229505. S2CID235758241.
↑Neal M, Barton Wright P (2003). "Validation therapy for dementia". The Cochrane Database of Systematic Reviews (3) CD001394. doi:10.1002/14651858.CD001394. PMID12917907.
↑Woods B, Aguirre E, Spector AE, etal. (February 2012). "Cognitive stimulation to improve cognitive functioning in people with dementia". The Cochrane Database of Systematic Reviews. 2 (2) CD005562. doi:10.1002/14651858.CD005562.pub2. PMID22336813. S2CID7086782.
↑Weitzel T, Robinson S, Barnes MR, etal. (2011). "The special needs of the hospitalized patient with dementia". Medsurg Nursing. 20 (1): 13–18, quiz 19. PMID21446290.
12Raj SE, Mackintosh S, Fryer C, etal. (January 1, 2021). "Home-Based Occupational Therapy for Adults With Dementia and Their Informal Caregivers: A Systematic Review". The American Journal of Occupational Therapy. 75 (1): 7501205060p1–7501205060p27. doi:10.5014/ajot.2020.040782. PMID33399054. S2CID230618534.
↑Lolk A, Gulmann NC (October 2006). "[Psychopharmacological treatment of behavioral and psychological symptoms in dementia]". Ugeskrift for Laeger (in Danish). 168 (40): 3429–3432. PMID17032610.
123Hadjistavropoulos T, Herr K, Turk DC, etal. (January 2007). "An interdisciplinary expert consensus statement on assessment of pain in older persons". The Clinical Journal of Pain. 23 (1 Suppl): S1–S43. doi:10.1097/AJP.0b013e31802be869. PMID17179836. S2CID43777445.
↑Stolee P, Hillier LM, Esbaugh J, etal. (February 2005). "Instruments for the assessment of pain in older persons with cognitive impairment". Journal of the American Geriatrics Society. 53 (2): 319–326. doi:10.1111/j.1532-5415.2005.53121.x. PMID15673359. S2CID21006144.
123456Alzheimer's Disease International (September 2015). "World Alzheimer Report 2015"(PDF). Archived(PDF) from the original on October 9, 2022. Retrieved October 30, 2018.
↑Sabayan B, Wyman-Chick KA, Sedaghat S (February 2023). "The Burden of Dementia Spectrum Disorders and Associated Comorbid and Demographic Features". Clinics in Geriatric Medicine. 39 (1): 1–14. doi:10.1016/j.cger.2022.07.001. PMID36404023. S2CID253068389.
↑Berrios GE (November 1987). "Dementia during the seventeenth and eighteenth centuries: a conceptual history". Psychological Medicine. 17 (4): 829–837. doi:10.1017/S0033291700000623. PMID3324141. S2CID8262492.
↑Berchtold NC, Cotman CW (1998). "Evolution in the conceptu-alization of dementia and Alzheimer's disease: Greco-Roman period to the 1960s". Neurobiol Aging. 19 (3): 173–189. doi:10.1016/s0197-4580(98)00052-9. PMID9661992. S2CID24808582.
↑Bergener M, Reisberg B (1989). Diagnosis and treatment of senile dementia. Berlin, Germany: Springer-Verlag. ISBN0-387-50800-7. OCLC19455117.
↑Xihua J (1989). Diagnosis and Treatment of Senile Dementia: Research Methods and Perspective. Madhav Books (P) Limited, a unit of Serials Publications. p.38. ISBN93-80615-34-5.
123Zilka, N., & Novak, M. (2006). The tangled story of Alois Alzheimer. Bratislavske lekarske listy, 107(9–10), 343–345.
↑Taylor DC. "Dementia". MedicineNet. Retrieved August 6, 2018. Senile dementia ("senility") is a term that was once used to describe all dementias; this term is no longer used as a diagnosis.
12Jia J, Wei C, Chen S, etal. (April 2018). "The cost of Alzheimer's disease in China and re-estimation of costs worldwide". Alzheimer's & Dementia. 14 (4): 483–491. doi:10.1016/j.jalz.2017.12.006. PMID29433981. S2CID46762069.
Husain M, Schott JM, eds. (2016). Oxford Textbook of Cognitive Neurology and Dementia. Oxford, England: Oxford University Press. ISBN978-0-19-883108-2. OCLC1081320148.
Lipton AM, Marshall CD (2013). The Common Sense Guide to Dementia for Clinicians and Caregivers. New York: Springer Publishing Company. ISBN978-1-4614-4162-5. OCLC788253522.
Mace NL, Rabins PV (2021). The 36-Hour Day (7thed.). Baltimore, Maryland: Johns Hopkins University Press. ISBN978-1-4214-4170-2. OCLC1260687360.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.