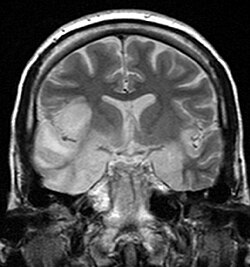
Limbic encephalitis refers to inflammatory disease confined to the limbic system of the brain. The clinical presentation often includes disorientation, disinhibition, memory loss, seizures, and behavioral anomalies. MRI imaging reveals T2 hyperintensity in the structures of the medial temporal lobes, and in some cases, other limbic structures. Some cases of limbic encephalitis are of autoimmune origin.[9]
Viral infections are the usual cause of infectious encephalitis.[11] Viral encephalitis can occur either as a direct effect of an acute infection, or as one of the sequelae of a latent infection. The majority of viral cases of encephalitis have an unknown cause; however, the most common identifiable cause of viral encephalitis is from herpes simplex infection.[12] Other causes of acute viral encephalitis are rabies virus, poliovirus, and measles virus.[13]
It can be caused by a bacterial infection, such as bacterial meningitis,[17] or may be a complication of a current infectious disease such as syphilis (secondary encephalitis).[18]
People should only be diagnosed with encephalitis if they have a decreased or altered level of consciousness, lethargy, or personality change for at least twenty-four hours without any other explainable cause.[23] Diagnosing encephalitis is done via a variety of tests:[24][25]
Brain scan, done by MRI, can determine inflammation and differentiate from other possible causes.
EEG, in monitoring brain activity, encephalitis will produce abnormal signal.
Lumbar puncture (spinal tap), this helps determine via a test using the cerebral-spinal fluid, obtained from the lumbar region.
An ideal drug to treat brain infection should be small, moderately lipophilic at pH of 7.4, low level of plasma protein binding, volume of distribution of litre per kg, does not have strong affinity towards binding with P-glycoprotein, or other efflux pumps on the surface of the blood–brain barrier. Some drugs such as isoniazid, pyrazinamide, linezolid, metronidazole, fluconazole, and some fluoroquinolones have good penetration of the blood brain barrier.[30] Treatment (which is based on supportive care) is as follows:[31]
Pyrimethamine-based maintenance therapy is often used to treat toxoplasmic encephalitis (TE), which is caused by Toxoplasma gondii and can be life-threatening for people with weak immune systems.[32] The use of highly active antiretroviral therapy (HAART), in conjunction with the established pyrimethamine-based maintenance therapy, decreases the chance of relapse in patients with HIV and TE from approximately 18% to 11%.[32] This is a significant difference as relapse may impact the severity and prognosis of disease and result in an increase in healthcare expenditure.[32]
The effectiveness of intravenousimmunoglobulin for the management of childhood encephalitis is unclear. Systematic reviews have been unable to draw firm conclusions because of a lack of randomiseddouble-blind studies with sufficient numbers of patients and sufficient follow-up.[33] There is the possibility of a benefit of intravenous immunoglobulin for some forms of childhood encephalitis on some indicators such as length of hospital stay, time to stop spasms, time to regain consciousness, and time to resolution of neuropathic symptoms and fever.[33] Intravenous immunoglobulin for Japanese encephalitis appeared to have no benefit when compared with placebo (pretend) treatment.[33]
The number of new cases a year of acute encephalitis in Western countries is 7.4 cases per 100,000 people per year. In tropical countries, the incidence is 6.34 per 100,000 people per year.[35] The number of cases of encephalitis has not changed much over time, with about 250,000 cases a year from 2005 to 2015 in the US. Approximately seven per 100,000 people were hospitalized for encephalitis in the US during this time.[34] In 2015, encephalitis was estimated to have affected 4.3million people and resulted in 150,000 deaths worldwide.[4][3] Herpes simplex encephalitis has an incidence of 2–4 per million of the population per year.[36]
The word is from Ancient Greekἐγκέφαλος, enképhalos 'brain',[37] composed of ἐν, en, 'in' and κεφαλή, kephalé, 'head', and the medical suffix -itis 'inflammation'.[38]
↑ Kneen R, Michael BD, Menson E, Mehta B, Easton A, Hemingway C, etal. (May 2012). "Management of suspected viral encephalitis in children - Association of British Neurologists and British Paediatric Allergy, Immunology and Infection Group national guidelines". The Journal of Infection. 64 (5): 449–477. doi:10.1016/j.jinf.2011.11.013. PMID22120594.
↑ "Japanese encephalitis". Immunization, Vaccines and Biologicals. World Health Organization. Archived from the original on 3 December 2013. Retrieved 2 April 2013.
↑ The word seems to have had a meaning of "lithic imitation of the human brain" at first, according to the Trésor de la langue française informatisé (cf. the article on "encéphalite"Archived 2017-11-05 at the Wayback Machine ). The first use in the medical sense is attested from the early 19th century in French (J. Capuron, Nouveau dictionnaire de médecine, chirurgie..., 1806), and from 1843 in English respectively (cf. the article "encephalitis" in the Online Etymology Dictionary). Retrieved 11 March 2017.
National Center for Biotechnology Information. "Encephalitis". PubMed Health. National Library of Medicine. Archived from the original on 2021-08-28. Retrieved 2015-08-05.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.