An arteriovenous malformation (AVM) is an abnormal connection between arteries and veins, bypassing the capillary system. Usually congenital, this vascular anomaly is widely known because of its occurrence in the central nervous system, but can appear anywhere in the body. The symptoms of AVMs can range from none at all to intense pain or bleeding, and they can lead to other serious medical problems.

A central venous catheter (CVC), also known as a central line (c-line), central venous line, or central venous access catheter, is a catheter placed into a large vein. It is a form of venous access. Placement of larger catheters in more centrally located veins is often needed in critically ill patients, or in those requiring prolonged intravenous therapies, for more reliable vascular access. These catheters are commonly placed in veins in the neck, chest, groin, or through veins in the arms.

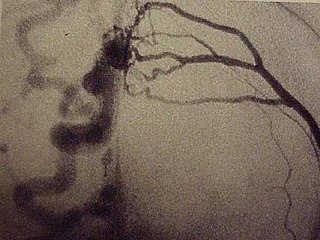
Angiography or arteriography is a medical imaging technique used to visualize the inside, or lumen, of blood vessels and organs of the body, with particular interest in the arteries, veins, and the heart chambers. Modern angiography is performed by injecting a radio-opaque contrast agent into the blood vessel and imaging using X-ray based techniques such as fluoroscopy.

Interventional radiology (IR) is a medical specialty that performs various minimally-invasive procedures using medical imaging guidance, such as x-ray fluoroscopy, computed tomography, magnetic resonance imaging, or ultrasound. IR performs both diagnostic and therapeutic procedures through very small incisions or body orifices. Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct. By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement, and angioplasty of narrowed structures.
Vascular surgery is a surgical subspecialty in which vascular diseases involving the arteries, veins, or lymphatic vessels, are managed by medical therapy, minimally-invasive catheter procedures and surgical reconstruction. The specialty evolved from general and cardiovascular surgery where it refined the management of just the vessels, no longer treating the heart or other organs. Modern vascular surgery includes open surgery techniques, endovascular techniques and medical management of vascular diseases - unlike the parent specialities. The vascular surgeon is trained in the diagnosis and management of diseases affecting all parts of the vascular system excluding the coronaries and intracranial vasculature. Vascular surgeons also are called to assist other physicians to carry out surgery near vessels, or to salvage vascular injuries that include hemorrhage control, dissection, occlusion or simply for safe exposure of vascular structures.

Hemodialysis, also spelled haemodialysis, or simply dialysis, is a process of filtering the blood of a person whose kidneys are not working normally. This type of dialysis achieves the extracorporeal removal of waste products such as creatinine and urea and free water from the blood when the kidneys are in a state of kidney failure. Hemodialysis is one of three renal replacement therapies. An alternative method for extracorporeal separation of blood components such as plasma or cells is apheresis.
A pseudoaneurysm, also known as a false aneurysm, is a locally contained hematoma outside an artery or the heart due to damage to the vessel wall. The injury passes through all three layers of the arterial wall, causing a leak, which is contained by a new, weak "wall" formed by the products of the clotting cascade. A pseudoaneurysm does not contain any layer of the vessel wall.

A dialysis catheter is a catheter used for exchanging blood to and from a hemodialysis machine and a patient.
Embolization refers to the passage and lodging of an embolus within the bloodstream. It may be of natural origin (pathological), in which sense it is also called embolism, for example a pulmonary embolism; or it may be artificially induced (therapeutic), as a hemostatic treatment for bleeding or as a treatment for some types of cancer by deliberately blocking blood vessels to starve the tumor cells.

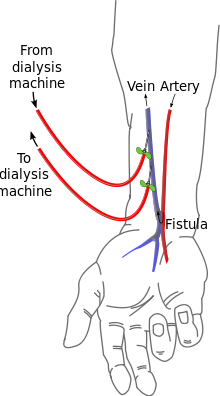
An arteriovenous fistula is an abnormal connection or passageway between an artery and a vein. It may be congenital, surgically created for hemodialysis treatments, or acquired due to pathologic process, such as trauma or erosion of an arterial aneurysm.

Hemofiltration, also haemofiltration, is a renal replacement therapy which is used in the intensive care setting. It is usually used to treat acute kidney injury (AKI), but may be of benefit in multiple organ dysfunction syndrome or sepsis. During hemofiltration, a patient's blood is passed through a set of tubing via a machine to a semipermeable membrane where waste products and water are removed by convection. Replacement fluid is added and the blood is returned to the patient.
Renal replacement therapy (RRT) is therapy that replaces the normal blood-filtering function of the kidneys. It is used when the kidneys are not working well, which is called kidney failure and includes acute kidney injury and chronic kidney disease. Renal replacement therapy includes dialysis, hemofiltration, and hemodiafiltration, which are various ways of filtration of blood with or without machines. Renal replacement therapy also includes kidney transplantation, which is the ultimate form of replacement in that the old kidney is replaced by a donor kidney.

A Cimino fistula, also Cimino-Brescia fistula, surgically created arteriovenous fistula and arteriovenous fistula, is a type of vascular access for hemodialysis. It is typically a surgically created connection between an artery and a vein in the arm, although there have been acquired arteriovenous fistulas which do not in fact demonstrate connection to an artery.
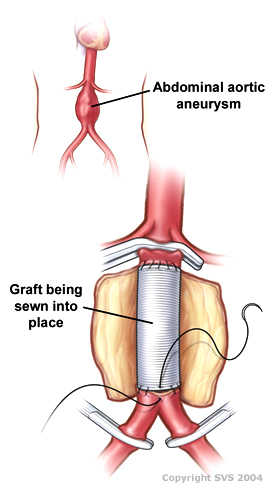
A vascular bypass is a surgical procedure performed to redirect blood flow from one area to another by reconnecting blood vessels. Often, this is done to bypass around a diseased artery, from an area of normal blood flow to another relatively normal area. It is commonly performed due to inadequate blood flow (ischemia) caused by atherosclerosis, as a part of organ transplantation, or for vascular access in hemodialysis. In general, someone's own vein (autograft) is the preferred graft material for a vascular bypass, but other types of grafts such as polytetrafluoroethylene (Teflon), polyethylene terephthalate (Dacron), or a different person's vein (allograft) are also commonly used. Arteries can also serve as vascular grafts. A surgeon sews the graft to the source and target vessels by hand using surgical suture, creating a surgical anastomosis.
A dural arteriovenous fistula (DAVF) or malformation is an abnormal direct connection (fistula) between a meningeal artery and a meningeal vein or dural venous sinus.
In nephrology, vascular access steal syndrome is a syndrome caused by ischemia resulting from a vascular access device that was installed to provide access for the inflow and outflow of blood during hemodialysis.

In medicine, a port is a small medical appliance that is installed beneath the skin. A catheter connects the port to a vein. Under the skin, the port has a septum through which drugs can be injected and blood samples can be drawn many times, usually with less discomfort for the patient than a more typical "needle stick".
The Nicoladoni–Branham sign is named after Carl Nicoladoni, who first noticed the phenomenon of the pulse slowing in a patient with right arm phlebarteriectasia when the brachialis artery proximal to it was compressed. In modern medicine, the sign is elicited when pressure is applied to an artery proximal to an arteriovenous fistula and said to be positive if the following occurs:
In medicine, vascular access is a means of accessing the bloodstream through the peripheral or central blood vessels in order to obtain blood or deliver medications including chemotherapy. A vascular access procedure involves insertion of a sterile plastic tube called a catheter into a blood vessel. Types of catheters can be either peripherally or centrally located. Peripheral catheters are approximately one inch (25 mm) long and are inserted into the small veins of the forearm. Central catheters are bigger and longer and are inserted into the large veins of the extremities, neck, or chest. Central venous catheters are the primary modality used for delivery of chemotherapeutic agents. The duration of central venous catheterization is dependent on the type of treatment given.
Ischemic monomelic neuropathy(IMN) is an uncommon vascular access complication in hemodialysis patients that manifests as multiple mononeuropathies without clinical ischemia. Ischemic monomelic neuropathy is most likely to affect patients who have had brachiocephalic vascular grafts, and it is characterized by symptoms of acute pain, numbness, and paresthesia in addition to motor weakness. The term "ischemic monomelic neuropathy" was first used in 1983 by Wilbourn, despite the fact that Bolton et al. had originally reported on it in 1979.