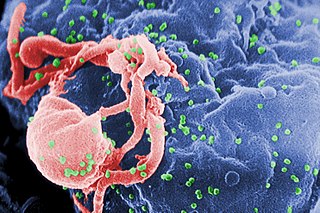
The human immunodeficiency viruses (HIV) are two species of Lentivirus that infect humans. Over time, they cause acquired immunodeficiency syndrome (AIDS), a condition in which progressive failure of the immune system allows life-threatening opportunistic infections and cancers to thrive. Without treatment, the average survival time after infection with HIV is estimated to be 9 to 11 years, depending on the HIV subtype.

A retrovirus is a type of virus that inserts a DNA copy of its RNA genome into the DNA of a host cell that it invades, thus changing the genome of that cell. After invading a host cell's cytoplasm, the virus uses its own reverse transcriptase enzyme to produce DNA from its RNA genome, the reverse of the usual pattern, thus retro (backwards). The new DNA is then incorporated into the host cell genome by an integrase enzyme, at which point the retroviral DNA is referred to as a provirus. The host cell then treats the viral DNA as part of its own genome, transcribing and translating the viral genes along with the cell's own genes, producing the proteins required to assemble new copies of the virus. Many retroviruses cause serious diseases in humans, other mammals, and birds.

Feline immunodeficiency virus (FIV) is a Lentivirus that affects cats worldwide, with 2.5% to 4.4% of felines being infected.

Adult T-cell leukemia/lymphoma is a rare cancer of the immune system's T-cells caused by human T cell leukemia/lymphotropic virus type 1 (HTLV-1). All ATL cells contain integrated HTLV-1 provirus further supporting that causal role of the virus in the cause of the neoplasm. A small amount of HTLV-1 individuals progress to develop ATL with a long latency period between infection and ATL development. ATL is categorized into 4 subtypes: acute, smoldering, lymphoma-type, chronic. Acute and Lymphoma-type are known to particularity be aggressive with poorer prognosis.
This is a list of AIDS-related topics, many of which were originally taken from the public domain U.S. Department of Health Glossary of HIV/AIDS-Related Terms, 4th Edition.

An oncovirus or oncogenic virus is a virus that can cause cancer. This term originated from studies of acutely transforming retroviruses in the 1950–60s, when the term "oncornaviruses" was used to denote their RNA virus origin. With the letters "RNA" removed, it now refers to any virus with a DNA or RNA genome causing cancer and is synonymous with "tumor virus" or "cancer virus". The vast majority of human and animal viruses do not cause cancer, probably because of longstanding co-evolution between the virus and its host. Oncoviruses have been important not only in epidemiology, but also in investigations of cell cycle control mechanisms such as the retinoblastoma protein.

Cutaneous T-cell lymphoma (CTCL) is a class of non-Hodgkin lymphoma, which is a type of cancer of the immune system. Unlike most non-Hodgkin lymphomas, CTCL is caused by a mutation of T cells. The cancerous T cells in the body initially migrate to the skin, causing various lesions to appear. These lesions change shape as the disease progresses, typically beginning as what appears to be a rash which can be very itchy and eventually forming plaques and tumors before spreading to other parts of the body.

Tropical spastic paraparesis (TSP), is a medical condition that causes weakness, muscle spasms, and sensory disturbance by human T-lymphotropic virus resulting in paraparesis, weakness of the legs. As the name suggests, it is most common in tropical regions, including the Caribbean. Blood transfusion products are screened for human T-lymphotropic virus 1 (HTLV-1) antibodies, as a preventive measure.

T-cell lymphoma is a rare form of cancerous lymphoma affecting T-cells. Lymphoma arises mainly from the uncontrolled proliferation of T-cells and can become cancerous.
A Tax Gene Product (Tax) is a nuclear protein that has a molecular weight of about 37,000 to 40,000 daltons.
Bovine leukemia virus (BLV) is a retrovirus which causes enzootic bovine leukosis in cattle. It is closely related to the human T‑lymphotropic virus type 1 (HTLV-I). BLV may integrate into the genomic DNA of B‑lymphocytes as a DNA intermediate, or exist as unintegrated circular or linear forms. Besides structural and enzymatic genes required for virion production, BLV expresses the Tax protein and microRNAs involved in cell proliferation and oncogenesis. In cattle, most infected animals are asymptomatic; leukemia is rare, but lymphoproliferation is more frequent (30%).
Robert Charles Gallo is an American biomedical researcher. He is best known for his role in establishing the human immunodeficiency virus (HIV) as the infectious agent responsible for acquired immune deficiency syndrome (AIDS) and in the development of the HIV blood test, and he has been a major contributor to subsequent HIV research.
Koala retrovirus (KoRV) is a retrovirus that is present in many populations of koalas. It has been implicated as the agent of koala immune deficiency syndrome (KIDS), an AIDS-like immunodeficiency that leaves infected koalas more susceptible to infectious disease and cancers. The virus is thought to be a recently introduced exogenous virus that is also integrating into the koala genome. Thus the virus can transmit both horizontally and vertically. The horizontal modes of transmission are not well defined but are thought to require close contact.

The primate T-lymphotropic viruses (PTLVs) are a group of retroviruses that infect primates, using their lymphocytes to reproduce. The ones that infect humans are known as human T-lymphotropic virus (HTLV), and the ones that infect Old World monkeys are called simian T-lymphotropic viruses (STLVs). PTLVs are named for their ability to cause adult T-cell leukemia/lymphoma, but in the case of HTLV-1 it can also cause a demyelinating disease called tropical spastic paraparesis. On the other hand, newer PTLVs are simply placed into the group by similarity and their connection to human disease remains unclear.

A virus closely related to HTLV-I, human T-lymphotropic virus 2 (HTLV-II) shares approximately 70% genomic homology with HTLV-I. It was discovered by Robert Gallo and colleagues.
Alexander F. Voevodin is a Russian-born biomedical scientist and educator. He is considered one of the leading early pioneers of HIV/AIDS research.
Viral synapse is a molecularly organized cellular junction that is similar in some aspects to immunological synapses. Many viruses including herpes simplex virus (HSV), human immunodeficiency virus (HIV) and human T-lymphotropic virus (HTLV) have been shown to instigate the formation of these junctions between the infected ("donor") and uninfected ("target") cell to allow cell-to-cell transmission. As viral synapses allow the virus to spread directly from cell to cell, they also provide a means by which the virus can escape neutralising antibody.
William "Bill" Fleming Hoggan Jarrett, RCVS, FRCPath, FRCPG, FRS (1928–2011) was a British pathologist.
Gibbon-ape leukemia virus (GaLV) is an oncogenic, type C retrovirus that has been isolated from primate neoplasms, including the white-handed gibbon and woolly monkey. The virus was identified as the etiological agent of hematopoietic neoplasms, leukemias, and immune deficiencies within gibbons in 1971, during the epidemic of the late 1960s and early 1970s. Epidemiological research into the origins of GaLV has developed two hypotheses for the virus' emergence. These include cross-species transmission of the retrovirus present within a species of East Asian rodent or bat, and the inoculation or blood transfusion of a MbRV-related virus into captured gibbons populations housed at medical research institutions. The virus was subsequently identified in captive gibbon populations in Thailand, the US and Bermuda.

Thomas A. Waldmann was an American immunologist who has worked on therapeutic monoclonal antibodies to the IL-2 receptor, Interleukin 15 (IL-15), and Adult T-cell Leukemia (ATL). Until the week he died, he was an active distinguished investigator at the Lymphoid Malignancies Branch of the National Cancer Institute.
