Methysergide is no longer recommended as a first line treatment protocol by international headache societies, hospitals, and neurologists in private practice, for migraines or cluster headaches as side effects were first reported with long-term use in the late 1960s, and ergot-based treatments fell out of favor for the treatment of migraines with the introduction of triptans in the 1980s.
Medical uses
Methysergide is used exclusively to treat episodic and chronic migraine and for episodic and chronic cluster headaches.[4] Methysergide is one of the most effective[5] medications for the prevention of migraine, but is not intended for the treatment of an acute attack, it is to be taken daily as a preventative medication.
Migraine and cluster headaches
Methysergide has been known as an effective treatment for migraine and cluster headache for over 50 years. A 2016 investigation by the European Medicines Agency due to long-held questions about safety concerns was performed. To assess the need for continuing availability of methysergide, the International Headache Society performed an electronic survey among their professional members.
The survey revealed that 71.3% of all respondents had ever prescribed methysergide and 79.8% would prescribe it if it were to become available. Respondents used it more in cluster headache than migraine, and reserved it for use in refractory patients.
The European Medicines Agency concluded "that the vast majority of headache experts in this survey regarded methysergide a unique treatment option for specific populations for which there are no alternatives, with an urgent need to continue its availability."
This position was supported by the International Headache Society.[6]
Updated guidelines published by Britain's National Health ServiceMigraine Trust in 2014 recommended "Methysergide medicines are now only to be used for preventing severe intractable migraine and cluster headache when standard medicines have failed".[7]
Methysergide antagonizes the effects of serotonin in blood vessels and gastrointestinal smooth muscle, but has few of the properties of other ergot alkaloids.[19] It is thought that metabolism of methysergide into methylergonovine is responsible for the antimigraine effects of methysergide.[20] Methylergonovine appears to be 10times more potent than methysergide as an agonist of the 5-HT1B and 5-HT1D receptors and has higher intrinsic efficacy in activating these receptors.[21] Methysergide produces psychedelic effects at high doses (3.5–7.5mg).[22]Metabolism of methysergide into methylergometrine is considered to be responsible for the psychedelic effects of methysergide.[18] The psychedelic effects can specifically be attributed to activation of the 5-HT2A receptor.[23] The medication can activate the 5-HT2B receptor due to metabolism into methylergometrine and for this reason has been associated with cardiac valvulopathy.[24][25] It is thought that the serotonin receptor antagonism of methysergide is not able to overcome the serotonin receptor agonism of methylergonovine due to the much higher levels of methylergonovine during methysergide therapy.[25]
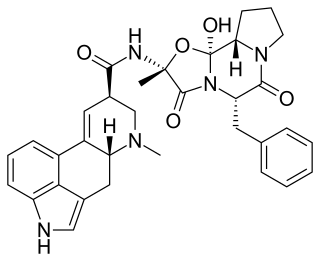
Methysergide, also known as N-[(2S)-1-hydroxybutan-2-yl]-1,6-dimethyl-9,10-didehydroergoline-8α-carboxamide or N-(1-(hydroxymethyl)propyl)-1-methyl-D-lysergamide, is a derivative of the ergolines and lysergamides and is structurally related to other members of these families, for instance lysergic acid diethylamide (LSD).
History
Harold Wolff's theory of vasodilation in migraine is well-known. Less known is his search for a perivascular factor that would damage local tissues and increase pain sensitivity during migraine attacks. Serotonin was found to be among the candidate agents to be included.
In the same period, serotonin was isolated (1948) and, because of its actions, an anti-serotonin drug was needed.
Methysergide was synthesized from lysergic acid by adding a methyl group and a butanolamid group. This resulted in a compound with selectivity and high potency as a serotonin (5-HT) inhibitor. Based on the possible involvement of serotonin in migraine attacks, it was introduced in 1959 by Sicuteri as a preventive drug for migraine. The clinical effect was often excellent, but 5 years later it was found to cause retroperitoneal fibrosis after chronic intake.
Consequently, the use of the drug in migraine declined considerably, but it was still used as a 5-HT antagonist in experimental studies. In 1974 Saxena showed that methysergide had a selective vasoconstrictor effect in the carotid bed and in 1984 he found an atypical receptor. This finding provided an incentive for the development of sumatriptan.[29]
Novartis withdrew it from the U.S. market after taking over Sandoz, but currently lists it as a discontinued product.[30]
Production and availability
US production of Methysergide, (Sansert), was discontinued on the manufacturer's own behalf in 2002. Sansert had previously been produced by Sandoz, which merged with Ciba-Geigy in 1996, and led to the creation of Novartis. In 2003 Novartis united its global generics businesses under a single global brand, with the Sandoz name and product line reviewed and reestablished.
Society and culture
Controversy
Methysergide has been an effective treatment for migraine and cluster headache for over 50 years but has systematically been suppressed from the migraine and cluster headache marketplace for over 15 years due to unqualified risk benefit/ratio safety concerns.[31]
Many cite the potential side effects of retroperitoneal/retropulmonary fibrosis as the prime reason methysergide is no longer frequently prescribed, but retroperitoneal fibrosis, and retropulmonary fibrosis, were documented as side effects as early as 1966,[32] and 1967,[33] respectively.
Related Research Articles
Ergotamine, sold under the brand names Cafergot and Ergomar among others, is an ergopeptine and part of the ergot family of alkaloids; it is structurally and biochemically closely related to ergoline. It is structurally similar to several neurotransmitters, and it acts as a vasoconstrictor.
Pergolide, sold under the brand name Permax and Prascend (veterinary) among others, is an ergoline-based dopamine receptor agonist used in some countries for the treatment of Parkinson's disease. Parkinson's disease is associated with reduced dopamine activity in the substantia nigra of the brain. Pergolide acts on many of the same receptors as dopamine to increase receptor activity.
5-HT receptors, 5-hydroxytryptamine receptors, or serotonin receptors, are a group of G protein-coupled receptor and ligand-gated ion channels found in the central and peripheral nervous systems. They mediate both excitatory and inhibitory neurotransmission. The serotonin receptors are activated by the neurotransmitter serotonin, which acts as their natural ligand.
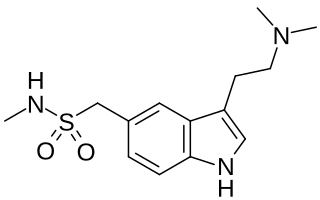
Triptans are a family of tryptamine-based drugs used as abortive medication in the treatment of migraines and cluster headaches. This drug class was first commercially introduced in the 1990s. While effective at treating individual headaches, they do not provide preventive treatment and are not considered a cure. They are not effective for the treatment of tension–type headache, except in persons who also experience migraines. Triptans do not relieve other kinds of pain.
Ergometrine, also known as ergonovine and sold under the brand names Ergotrate, Ergostat, and Syntometrine among others, is a medication used to cause contractions of the uterus to treat heavy vaginal bleeding after childbirth. It can be used either by mouth, by injection into a muscle, or injection into a vein. It begins working within 15 minutes when taken by mouth and is faster in onset when used by injection. Effects last between 45 and 180 minutes.
Dihydroergotamine (DHE), sold under the brand names D.H.E. 45 and Migranal among others, is an ergot alkaloid used to treat migraines. It is a derivative of ergotamine. It is administered as a nasal spray or injection and has an efficacy similar to that of sumatriptan. Nausea is a common side effect.
Methylergometrine, also known as methylergonovine and sold under the brand name Methergine, is a medication of the ergoline and lysergamide groups which is used as an oxytocic in obstetrics and in the treatment of migraine. It reportedly produces psychedelic effects similar to those of lysergic acid diethylamide (LSD) at high doses.
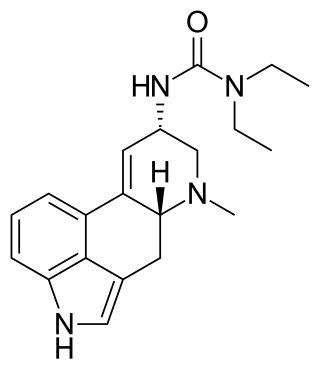
Lisuride, sold under the brand name Dopergin among others, is a monoaminergic medication of the ergoline class which is used in the treatment of Parkinson's disease, migraine, and high prolactin levels. It is taken by mouth.
The 5-HT2A receptor is a subtype of the 5-HT2 receptor that belongs to the serotonin receptor family and is a G protein-coupled receptor (GPCR). The 5-HT2A receptor is a cell surface receptor, but has several intracellular locations.
A serotonin receptor agonist is an agonist of one or more serotonin receptors. They activate serotonin receptors in a manner similar to that of serotonin, a neurotransmitter and hormone and the endogenous ligand of the serotonin receptors.
meta-Chlorophenylpiperazine (mCPP) is a psychoactive drug of the phenylpiperazine class. It was initially developed in the late-1970s and used in scientific research before being sold as a designer drug in the mid-2000s. It has been detected in pills touted as legal alternatives to illicit stimulants in New Zealand and pills sold as "ecstasy" in Europe and the United States.
Cardiac fibrosis commonly refers to the excess deposition of extracellular matrix in the cardiac muscle, but the term may also refer to an abnormal thickening of the heart valves due to inappropriate proliferation of cardiac fibroblasts. Fibrotic cardiac muscle is stiffer and less compliant and is seen in the progression to heart failure. The description below focuses on a specific mechanism of valvular pathology but there are other causes of valve pathology and fibrosis of the cardiac muscle.
A serotonin antagonist, or serotonin receptor antagonist, is a drug used to inhibit the action of serotonin and serotonergic drugs at serotonin (5-HT) receptors.
5-Hydroxytryptamine receptor 2B (5-HT2B) also known as serotonin receptor 2B is a protein that in humans is encoded by the HTR2B gene. 5-HT2B is a member of the 5-HT2 receptor family that binds the neurotransmitter serotonin (5-hydroxytryptamine, 5-HT). Like all 5-HT2 receptors, the 5-HT2B receptor is Gq/G11-protein coupled, leading to downstream activation of phospholipase C.
Terguride, sold under the brand name Teluron, is a serotonin receptor antagonist and dopamine receptor agonist of the ergoline family. It is approved for and used as a prolactin inhibitor in the treatment of hyperprolactinemia in Japan. Terguride is taken by mouth.
A serotonin releasing agent (SRA) is a type of drug that induces the release of serotonin into the neuronal synaptic cleft. A selective serotonin releasing agent (SSRA) is an SRA with less significant or no efficacy in producing neurotransmitter efflux at other types of monoamine neurons.
5-HT2C receptor agonists are a class of drugs that activate 5-HT2C receptors. They have been investigated for the treatment of a number of conditions including obesity, psychiatric disorders, sexual dysfunction and urinary incontinence.
25CN-NBOH is a compound indirectly derived from the phenethylamine series of hallucinogens, which was discovered in 2014 at the University of Copenhagen. This compound is notable as one of the most selective agonist ligands for the 5-HT2A receptor yet discovered, with a pKi of 8.88 at the human 5-HT2A receptor and with 100x selectivity for 5-HT2A over 5-HT2C, and 46x selectivity for 5-HT2A over 5-HT2B. A tritiated version of 25CN-NBOH has also been accessed and used for more detailed investigations of the binding to 5-HT2 receptors and autoradiography.
1-Methylpsilocin is a tryptamine derivative which acts as a selective agonist for the 5-HT2C receptor (IC50 of 12 nM, vs 633 nM at 5-HT2A), and an inverse agonist at 5-HT2B (Ki of 38 nM). While 1-methylpsilocin does have higher affinity for 5-HT2C than 5-HT2A, it does produce a head-twitch response in mice that are dependent on 5-HT2A, so it is not entirely free of effects on 5-HT2A in vivo. In contrast to psilocin, 1-methylpsilocin did not activate 5-HT1A receptors in mice. 1-Methylpsilocin has been investigated for applications such as treatment of glaucoma, OCD, and cluster headaches, as these conditions are amenable to treatment with psychedelic drugs but are not generally treated with such agents due to the hallucinogenic side effects they produce, which are considered undesirable. 1-Methylpsilocin therefore represents a potential alternative treatment to psilocin that may be less likely to produce hallucinogenic effects.
Donitriptan (INN) is a triptan drug which was investigated as an antimigraine agent but ultimately was never marketed. It acts as a high-affinity, high-efficacy/near-full agonist of the 5-HT1B and 5-HT1D receptors, and is among the most potent of the triptan series of drugs. Donitriptan was being developed in France by bioMérieux-Pierre Fabre and made it to phase II clinical trials in Europe before development was discontinued.
1 2 3 4 5 Ramírez Rosas MB, Labruijere S, Villalón CM, Maassen Vandenbrink A (August 2013). "Activation of 5-hydroxytryptamine1B/1D/1F receptors as a mechanism of action of antimigraine drugs". Expert Opinion on Pharmacotherapy. 14 (12): 1599–1610. doi:10.1517/14656566.2013.806487. PMID23815106. S2CID22721405.
1 2 Joseph T, Tam SK, Kamat BR, Mangion JR (April 2003). "Successful repair of aortic and mitral incompetence induced by methylsergide maleate: confirmation by intraoperative transesophageal echocardiography". Echocardiography. 20 (3): 283–287. doi:10.1046/j.1540-8175.2003.03027.x. PMID12848667. S2CID22513342.
↑ MacGregor EA, Evers S (October 2017). "The role of methysergide in migraine and cluster headache treatment worldwide - A survey in members of the International Headache Society". Cephalalgia. 37 (11): 1106–1108. doi:10.1177/0333102416660551. PMID27449673. S2CID206521928.
↑ Rang HP (2003). Pharmacology. Edinburgh: Churchill Livingstone. ISBN978-0-443-07145-4. Page 187
↑ Saxena PR, Lawang A (October 1985). "A comparison of cardiovascular and smooth muscle effects of 5-hydroxytryptamine and 5-carboxamidotryptamine, a selective agonist of 5-HT1 receptors". Archives Internationales de Pharmacodynamie et de Therapie. 277 (2): 235–252. PMID2933009.
↑ Colpaert FC, Niemegeers CJ, Janssen PA (October 1979). "In vivo evidence of partial agonist activity exerted by purported 5-hydroxytryptamine antagonists". European Journal of Pharmacology. 58 (4): 505–509. doi:10.1016/0014-2999(79)90326-1. PMID510385.
1 2 Knight AR, Misra A, Quirk K, Benwell K, Revell D, Kennett G, Bickerdike M (August 2004). "Pharmacological characterisation of the agonist radioligand binding site of 5-HT(2A), 5-HT(2B) and 5-HT(2C) receptors". Naunyn-Schmiedeberg's Archives of Pharmacology. 370 (2): 114–123. doi:10.1007/s00210-004-0951-4. PMID15322733. S2CID8938111.
1 2 3 Fitzgerald LW, Burn TC, Brown BS, Patterson JP, Corjay MH, Valentine PA, etal. (January 2000). "Possible role of valvular serotonin 5-HT(2B) receptors in the cardiopathy associated with fenfluramine". Molecular Pharmacology. 57 (1): 75–81. PMID10617681.
1 2 Bredberg U, Eyjolfsdottir GS, Paalzow L, Tfelt-Hansen P, Tfelt-Hansen V (1 January 1986). "Pharmacokinetics of methysergide and its metabolite methylergometrine in man". European Journal of Clinical Pharmacology. 30 (1): 75–77. doi:10.1007/BF00614199. PMID3709634. S2CID9583732.
↑ "methysergide". PubChem. U.S. National Library of Medicine. Retrieved 2017-09-06.
1 2 3 4 Majrashi M, Ramesh S, Deruiter J, Mulabagal V, Pondugula S, Clark R, Dhanasekaran M (2017). "Multipotent and Poly-therapeutic Fungal Alkaloids of Claviceps purpurea". In Agrawal DC, Tsay HS, Shyur LF, Wu YC, Wang SY (eds.). Medicinal Plants and Fungi: Recent Advances in Research and Development. Medicinal and Aromatic Plants of the World. Vol.4. pp.229–252. doi:10.1007/978-981-10-5978-0_8. ISBN978-981-10-5977-3. ISSN2352-6831.
↑ Graham JR, Suby HI, LeCompte PR, Sadowsky NL (February 1966). "Fibrotic disorders associated with methysergide therapy for headache". The New England Journal of Medicine. 274 (7): 359–368. doi:10.1056/NEJM196602172740701. PMID5903120.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.