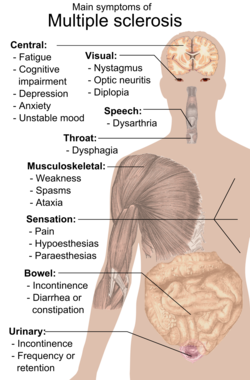
The initial attacks are often transient, mild (or asymptomatic), and self-limited. They often do not prompt a health care visit and sometimes are only identified in retrospect once the diagnosis has been made after further attacks. The most common initial symptoms reported are: changes in sensation in the arms, legs or face (33%), complete or partial vision loss (optic neuritis) (20%), weakness (13%), double vision (7%), unsteadiness when walking (5%), and balance problems (3%); but many rare initial symptoms have been reported such as aphasia or psychosis.[2][3] Fifteen percent of individuals have multiple symptoms when they first seek medical attention.[4]
Fatigue
Fatigue is very common[5] and disabling in MS.[6][7] Some 65% of people with MS experience fatigue symptomatology, and of these some 15-40% report fatigue as their most disabling MS symptom.[8]
Primary vs. secondary
In some areas it has been proposed that fatigue be separated into primary fatigue, caused directly by a disease process, and secondary fatigue, caused by more general impacts on the person of having a disease (such as disrupted sleep).[9][10][11][12]
Contributory factors to secondary fatigue
Factors such as disturbed sleep, chronic pain, poor nutrition, or even some medications can all contribute to secondary fatigue and medical professionals are encouraged to identify and modify them.[13] There are also different medications used to treat fatigue such as amantadine,[14][15]pemoline,[16][17]methylphenidate, and modafinil,[18] as well as cognitive behavioral therapy (CBT) and psychological interventions of energy conservation;[19][20] but their effects are limited.[18] For these reasons fatigue is a difficult symptom to manage. Fatigue has also been related to specific brain areas in MS using magnetic resonance imaging.[21]
Association with depression
Early 2000s commentary saw a close relationship of secondary fatigue with depressive symptomatology.[22] When depression is reduced fatigue also tends to reduce and it is recommended that patients should be evaluated for depression before other therapeutic approaches are used.[23]
Bladder and bowel
Bladder problems (See also urinary system and urination) appear in 70–80% of people with multiple sclerosis (MS) and they have an important effect both on hygiene habits and social activity.[24][25] Bladder problems are usually related with high levels of disability and pyramidal signs in lower limbs.[26]
The most common problems are an increase in frequency and urgency (incontinence) but difficulties to begin urination, hesitation, leaking, sensation of incomplete urination, and retention also appear. When retention occurs secondary urinary infections are common.
Treatment objectives are the alleviation of symptoms of urinary dysfunction, treatment of urinary infections, reduction of complicating factors and the preservation of renal function. Treatments can be classified in two main subtypes: pharmacological and non-pharmacological. Pharmacological treatments vary greatly depending on the origin or type of dysfunction and some examples of the medications used are:[28]alfuzosin for retention,[29]trospium and flavoxate for urgency and incontinency,[30][31] and desmopressin for nocturia.[32][33] Non pharmacological treatments involve the use of pelvic floor muscle training, stimulation, biofeedback, pessaries, bladder retraining, and sometimes intermittent catheterization.[34][35]
Bowel problems affect around 70% of patients. Around 50% of patients experience constipation and up to 30% experience fecal incontinence.[35] Cause of bowel impairments in MS patients is usually either a reduced gut motility or an impairment in neurological control of defecation. The former is commonly related to immobility or secondary effects from drugs used in the treatment of the disease.[35] Pain or problems with defecation can be helped with a diet change which includes among other changes an increased fluid intake, oral laxatives or suppositories and enemas when habit changes and oral measures are not enough to control the problems.[35][36]
Cognitive
Some of the most common deficits affect recent memory, attention, processing speed, visual-spatial abilities and executive function.[37] Symptoms related to cognition include emotional instability and fatigue including neurological fatigue. Commonly a form of cognitive disarray is experienced, where specific cognitive processes may remain unaffected, but cognitive processes as a whole are impaired. Cognitive deficits are independent of physical disability and can occur in the absence of neurological dysfunction.[38] Severe impairment is a major predictor of a low quality of life, unemployment, caregiver distress,[39] and difficulty in driving;[40] limitations in a patient's social and work activities are also correlated with the extent of impairment.[38]
Cognitive impairments occur in about 40 to 60 percent of patients with multiple sclerosis,[41] with the lowest percentages usually from community-based studies and the highest ones from hospital-based. Impairments may be present at the beginning of the disease.[42] Probable multiple sclerosis patients, meaning after a first attack but before a secondary confirmatory one, have up to 50 percent of patients with impairment at onset.[43]Dementia is rare and occurs in only five percent of patients.[38]
Measures of tissue atrophy are well correlated with, and predict, cognitive dysfunction. Neuropsychological outcomes are highly correlated with linear measures of sub-cortical atrophy. Cognitive impairment is the result of not only tissue damage,[44] but tissue repair and adaptive functional reorganization.[39]Neuropsychological testing is important for determining the extent of cognitive deficits. Neuropsychological rehabilitation may help to reverse or decrease the cognitive deficits although studies on the issue have been of low quality.[45]Acetylcholinesterase inhibitors are commonly used to treat Alzheimer's disease related dementia and so are thought to have potential in treating the cognitive deficits in multiple sclerosis. They have been found to be effective in preliminary clinical trials.[45]
Emotional
Emotional symptoms are also common and are thought to be both a normal response to having a debilitating disease and the result of damage to specific areas of the central nervous system that generate and control emotions.[citation needed]
Clinical depression is the most common neuropsychiatric condition: lifetime depression prevalence rates of 40–50% and 12-month prevalence rates around 20% have been typically reported for samples of people with MS; these figures are considerably higher than those for the general population or for people with other chronic illnesses.[46][47] Brain imaging studies trying to relate depression to lesions in certain regions of the brain have met with variable success. On balance the evidence seems to favour an association with neuropathology in the left anterior temporal/parietal regions.[48]
Other feelings such as anger, anxiety, frustration, and hopelessness also appear frequently. Suicide is a possibility, since it accounts for 15% of MS deaths.[49]
Internuclear ophthalmoplegia is a disorder of conjugate lateral gaze. The affected eye shows impairment of adduction. The partner eye diverges from the affected eye during abduction, producing diplopia; during extreme abduction, compensatory nystagmus can be seen in the partner eye. Diplopia means double vision while nystagmus is involuntary eye movement characterized by alternating smooth pursuit in one direction and a saccadic movement in the other direction.[citation needed]
Internuclear ophthalmoplegia occurs when MS affects a part of the brain stem called the medial longitudinal fasciculus, which is responsible for communication between the two eyes by connecting the abducens nucleus of one side to the oculomotor nucleus of the opposite side. This results in the failure of the medial rectus muscle to contract appropriately, so that the eyes do not move equally (called disconjugate gaze).[citation needed]
Different drugs as well as optic compensatory systems and prisms can be used to improve these symptoms.[51][52][53][54] Surgery can also be used in some cases for this problem.[55]
Mobility restrictions
Animation created from an 1887 photographic study of locomotion of a male MS patient with walking difficulties by Muybridge
Restrictions in mobility (walking, transfers, bed mobility etc.) are common in individuals with multiple sclerosis. Although this is not something constant it can happen when experiencing a flare up. Within 10 years after the onset of MS one-third of patients reach a score of 6 on the Expanded Disability Status Scale (EDSS), requiring the use of a unilateral walking aid, and by 30 years the proportion increases to 83%. Within five years of onset the EDSS is six in 50% of those with the progressive form of MS.[56]
A wide range of impairments may exist in people with MS, which can act either alone or in combination to impact directly on a person's balance, function and mobility. Such impairments include fatigue, weakness, hypertonicity, low exercise tolerance, impaired balance, ataxia and tremor.[57]
Interventions may be aimed at the individual impairments that reduce mobility or at the level of disability. This second level intervention includes provision, education, and instruction in the use of equipment such as walking aids, wheelchairs, motorized scooters and car adaptations as well as instruction on compensatory strategies to accomplish an activity — for example undertaking safe transfers by pivoting in a flexed posture rather than standing up and stepping around.
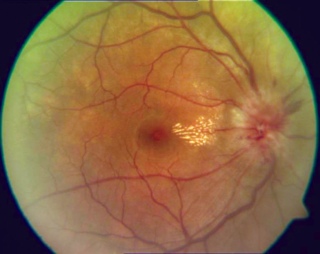
Up to 50% of patients with MS will develop an episode of optic neuritis and 20% of the time optic neuritis is the presenting sign of MS. The presence of demyelinating white matter lesions on brain MRIs at the time of presentation for optic neuritis is the strongest predictor in developing clinical diagnosis of MS. Almost half of patients with optic neuritis have white matter lesions consistent with multiple sclerosis.
At five year follow-ups the overall risk of developing MS is 30%, with or without MRI lesions. Patients with a normal MRI still develop MS (16%), but at a lower rate compared to those patients with three or more MRI lesions (51%). From the other perspective, however, 44% of patients with any demyelinating lesions on MRI at presentation will not have developed MS ten years later.[58][59]
Individuals experience rapid onset of pain in one eye followed by blurry vision in part or all its visual field. Flashes of light (phosphenes) may also be present.[60]Inflammation of the optic nerve causes loss of vision most usually by the swelling and destruction of the myelin sheath covering the optic nerve.
The blurred vision usually resolves within 10 weeks but individuals are often left with less vivid color vision, especially red, in the affected eye.[citation needed]
A systemic intravenous treatment with corticosteroids may quicken the healing of the optic nerve, prevent complete loss of vision and delay the onset of other symptoms.[citation needed]
Pain
Pain is a common symptom in MS. A recent study systematically pooling results from 28 studies (7101 patients) estimates that pain affects 63% of people with MS.[61] These 28 studies described pain in a large range of different people with MS. The authors found no evidence that pain was more common in people with progressive types of MS, in females compared to males, in people with different levels of disability, or in people who had had MS for different periods of time.
Pain can be severe and debilitating, and can have a profound effect on the quality of life and mental health of those affected.[62] Certain types of pain are thought to sometimes appear after a lesion to the ascending or descending tracts that control the transmission of painful stimulus, such as the anterolateral system, but many other causes are also possible.[53] The most prevalent types of pain are thought to be headaches (43%), dysesthetic limb pain (26%), back pain (20%), painful spasms (15%) such as the MS Hug,[63] painful Lhermitte's phenomenon (16%) and Trigeminal Neuralgia (3%).[61] These authors did not however find enough data to quantify the prevalence of painful optic neuritis.
Trigeminal neuralgia (or "tic douloureux") is a disorder of the trigeminal nerve that causes episodes of intense pain in the eyes, lips, nose, scalp, forehead, and jaw, affecting 2-4% of MS patients.[61] The episodes of pain occur paroxysmally (suddenly) and the patients describe it as trigger area on the face, so sensitive that touching or even air currents can bring an episode of pain. Usually it is successfully treated with anticonvulsants such as carbamazepine,[65] or phenytoin[66] although others such as gabapentin[67] can be used.[68] When drugs are not effective, surgery may be recommended. Glycerol rhizotomy (surgical injection of glycerol into a nerve) has been studied[69] although the beneficial effects and risks in MS patients of the procedures that relieve pressure on the nerve are still under discussion.[70][71]
Lhermitte's sign
Lhermitte's sign is an electrical sensation that runs down the back and into the limbs and is produced by bending the neck forward. The sign suggests a lesion of the dorsal columns of the cervical cord or of the caudal medulla, correlating significantly with cervical MRI abnormalities.[72] Between 25 and 40% of MS patients report having Lhermitte's sign during the course of their illness.[73][74][75] It is not always experienced as painful, but about 16% of people with MS will experience painful Lhermitte's sign.[61]
Dysesthesias
Dysesthesias are disagreeable sensations produced by ordinary stimuli. The abnormal sensations are caused by lesions of the peripheral or central sensory pathways, and are described as painful feelings such as burning, wetness, itching, electric shock or pins and needles. Both Lhermitte's sign and painful dysesthesias usually respond well to treatment with carbamazepine, clonazepam or amitriptyline.[76][77][78] A related symptom is a pleasant, yet unsettling sensation which has no normal explanation (such as sensation of gentle warmth arising from touch by clothing)[citation needed]
Reduced sense of smell
People with Multiple Sclerosis have been found to have reduced sense of smell, including lower olfactory thresholds.[79][80][81]
Sexual
Sexual dysfunction (SD) is one of many symptoms affecting persons with a diagnosis of MS. SD in men encompasses both erectile and ejaculatory disorder. The prevalence of SD in men with MS ranges from 75 to 91%.[82] Erectile dysfunction appears to be the most common form of SD documented in MS. SD may be due to alteration of the ejaculatory reflex which can be affected by neurological conditions such as MS.[83] Sexual dysfunction is also prevalent in female MS patients, typically lack of orgasm, probably related to disordered genital sensation.
Spasticity
Photographic study of locomotion of a MS female patient with walking difficulties and spasticity created in 1887 by Muybridge
Spasticity is characterized by increased stiffness and slowness in limb movement, the development of certain postures, an association with weakness of voluntary muscle power, and with involuntary and sometimes painful spasms of limbs.[13] Painful spasms affect about 15% of people with MS overall.[61] A physiotherapist can help to reduce spasticity and avoid the development of contractures with techniques such as passive stretching.[84] There is evidence, albeit limited, of the clinical effectiveness of THC and CBD extracts,[85]baclofen,[86]dantrolene,[87]diazepam,[88] and tizanidine.[89][90][91] In the most complicated cases intrathecal injections of baclofen can be used.[92] There are also palliative measures like castings, splints or customized seatings.[13]
Speech and swallowing
Speech problems include slurred speech, low tone of voice (dysphonia), decreased talking speed, and problems with articulation of sounds (dysarthria).
A related problem, since it involves similar anatomical structures, is swallowing difficulties (dysphagia).[93]
Some MS patients develop rapid onset of numbness, weakness, bowel or bladder dysfunction, and/or loss of muscle function, typically in the lower half of the body.[citation needed] This is the result of MS attacking the spinal cord. The symptoms and signs depend upon the nerve cords involved and the extent of the involvement.
Prognosis for complete recovery is generally poor. Recovery from transverse myelitis usually begins between weeks 2 and 12 following onset and may continue for up to 2 years in some patients and as many as 80% of individuals with transverse myelitis are left with lasting disabilities.[citation needed]
Though it was considered for many years that traverse myelitis was a normal consequence of MS, since the discovery of anti-AQP4 and anti-MOG biomarkers it is not. Now TM is considered an indicator of neuromyelitis optica, and a red flag against the diagnosis of MS.[94]
Tremor is an unintentional, somewhat rhythmic, muscle movement involving to-and-fro movements (oscillations) of one or more parts of the body. It is the most common of all involuntary movements and can affect the hands, arms, head, face, vocal cords, trunk, and legs. Ataxia is an unsteady and clumsy motion of the limbs or torso due to a failure of the gross coordination of muscle movements. People with ataxia experience a failure of muscle control in their arms and legs, resulting in a lack of balance and coordination or a disturbance of gait.
Tremor and ataxia are frequent in MS and present in 25 to 60% of patients. They can be very disabling and embarrassing, and are difficult to manage.[95] The origin of tremor in MS is difficult to identify but it can be due to a mixture of different factors such as damage to the cerebellar connections, weakness, spasticity, etc.
Many medications have been proposed to treat tremor; however their efficacy is very limited. Medications that have been reported to provide some relief are isoniazid,[96][97][98][99]carbamazepine,[65]propranolol[100][101][102] and gluthetimide[103] but published evidence of effectiveness is limited.[104]Physical therapy is not indicated as a treatment for tremor or ataxia although the use of orthese devices can help. An example is the use of wrist bandages with weights, which can be useful to increase the inertia of movement and therefore reduce tremor.[105] Daily use objects are also adapted so they are easier to grab and use.
If all these measures fail patients are candidates for thalamussurgery. This kind of surgery can be both a thalamotomy or the implantation of a thalamic stimulator. Complications are frequent (30% in thalamotomy and 10% in deep brain stimulation) and include a worsening of ataxia, dysarthria and hemiparesis. Thalamotomy is a more efficacious surgical treatment for intractable MS tremor though the higher incidence of persistent neurological deficits in patients receiving lesional surgery supports the use of deep brain stimulation as the preferred surgical strategy.[106]
Related Research Articles
Acute disseminated encephalomyelitis (ADEM), or acute demyelinating encephalomyelitis, is a rare autoimmune disease marked by a sudden, widespread attack of inflammation in the brain and spinal cord. As well as causing the brain and spinal cord to become inflamed, ADEM also attacks the nerves of the central nervous system and damages their myelin insulation, which, as a result, destroys the white matter. The cause is often a trigger such as from viral infection or vaccinations.
Optic neuritis describes any condition that causes inflammation of the optic nerve; it may be associated with demyelinating diseases, or infectious or inflammatory processes.
Transverse myelitis (TM) is a rare neurological condition wherein the spinal cord is inflamed. The adjective transverse implies that the spinal inflammation (myelitis) extends horizontally throughout the cross section of the spinal cord; the terms partial transverse myelitis and partial myelitis are sometimes used to specify inflammation that affects only part of the width of the spinal cord. TM is characterized by weakness and numbness of the limbs, deficits in sensation and motor skills, dysfunctional urethral and anal sphincter activities, and dysfunction of the autonomic nervous system that can lead to episodes of high blood pressure. Signs and symptoms vary according to the affected level of the spinal cord. The underlying cause of TM is unknown. The spinal cord inflammation seen in TM has been associated with various infections, immune system disorders, or damage to nerve fibers, by loss of myelin. As opposed to leukomyelitis which affects only the white matter, it affects the entire cross-section of the spinal cord. Decreased electrical conductivity in the nervous system can result.
Multiple sclerosis (MS) is an autoimmune disease in which the insulating covers of nerve cells in the brain and spinal cord are damaged. This damage disrupts the ability of parts of the nervous system to transmit signals, resulting in a range of signs and symptoms, including physical, mental, and sometimes psychiatric problems. Specific symptoms can include double vision, vision loss, eye pain, muscle weakness, and loss of sensation or coordination. MS takes several forms, with new symptoms either occurring in isolated attacks or building up over time. In the relapsing forms of MS, between attacks, symptoms may disappear completely, although some permanent neurological problems often remain, especially as the disease advances. In the progressive forms of MS, bodily function slowly deteriorates and disability worsens once symptoms manifest and will steadily continue to do so if the disease is left untreated.
A demyelinating disease refers to any disease affecting the nervous system where the myelin sheath surrounding neurons is damaged. This damage disrupts the transmission of signals through the affected nerves, resulting in a decrease in their conduction ability. Consequently, this reduction in conduction can lead to deficiencies in sensation, movement, cognition, or other functions depending on the nerves affected.
Neuromyelitis optica spectrum disorders (NMOSD) are a spectrum of autoimmune diseases characterized by acute inflammation of the optic nerve and the spinal cord (myelitis). Episodes of ON and myelitis can be simultaneous or successive. A relapsing disease course is common, especially in untreated patients.
Interferon beta-1b is a cytokine in the interferon family used to treat the relapsing-remitting and secondary-progressive forms of multiple sclerosis (MS). It is approved for use after the first MS event. Closely related is interferon beta 1a, also indicated for MS, with a very similar drug profile.
Neuritis, from the Greek νεῦρον), is inflammation of a nerve or the general inflammation of the peripheral nervous system. Inflammation, and frequently concomitant demyelination, cause impaired transmission of neural signals and leads to aberrant nerve function. Neuritis is often conflated with neuropathy, a broad term describing any disease process which affects the peripheral nervous system. However, neuropathies may be due to either inflammatory or non-inflammatory causes, and the term encompasses any form of damage, degeneration, or dysfunction, while neuritis refers specifically to the inflammatory process.
Uhthoff's phenomenon is the worsening of neurologic symptoms in multiple sclerosis (MS) and other demyelinating diseases when the body is overheated. This may occur due to hot weather, exercise, fever, saunas, hot tubs, hot baths, and hot food and drink. Increased temperature slows nerve conduction, but the exact mechanism remains unknown. With an increased body temperature, nerve impulses are either blocked or slowed in a damaged nerve. Once the body temperature is normalized, signs and symptoms typically reverse.
Intention tremor is a dyskinetic disorder characterized by a broad, coarse, and low-frequency tremor evident during deliberate and visually-guided movement. An intention tremor is usually perpendicular to the direction of movement. When experiencing an intention tremor, one often overshoots or undershoots one's target, a condition known as dysmetria. Intention tremor is the result of dysfunction of the cerebellum, particularly on the same side as the tremor in the lateral zone, which controls visually guided movements. Depending on the location of cerebellar damage, these tremors can be either unilateral or bilateral.
Multiple sclerosis is an inflammatory demyelinating disease of the CNS in which activated immune cells invade the central nervous system and cause inflammation, neurodegeneration, and tissue damage. The underlying cause is currently unknown. Current research in neuropathology, neuroimmunology, neurobiology, and neuroimaging, together with clinical neurology, provide support for the notion that MS is not a single disease but rather a spectrum.
Multiple sclerosis (MS) is a chronic inflammatory demyelinating disease that affects the central nervous system (CNS). Several therapies for it exist, although there is no known cure.
Inflammatory demyelinating diseases (IDDs), sometimes called Idiopathic (IIDDs) due to the unknown etiology of some of them, are a heterogenous group of demyelinating diseases - conditions that cause damage to myelin, the protective sheath of nerve fibers - that occur against the background of an acute or chronic inflammatory process. IDDs share characteristics with and are often grouped together under Multiple Sclerosis. They are sometimes considered different diseases from Multiple Sclerosis, but considered by others to form a spectrum differing only in terms of chronicity, severity, and clinical course.
Tumefactive multiple sclerosis is a condition in which the central nervous system of a person has multiple demyelinating lesions with atypical characteristics for those of standard multiple sclerosis (MS). It is called tumefactive as the lesions are "tumor-like" and they mimic tumors clinically, radiologically and sometimes pathologically.
Signs and symptoms of Parkinson's disease are varied. Parkinson's disease affects movement, producing motor symptoms. Non-motor symptoms, which include dysautonomia, cognitive and neurobehavioral problems, and sensory and sleep difficulties, are also common. When other diseases mimic Parkinson's disease, they are categorized as parkinsonism.
Schumacher criteria are diagnostic criteria that were previously used for identifying multiple sclerosis (MS). Multiple sclerosis, understood as a central nervous system (CNS) condition, can be difficult to diagnose since its signs and symptoms may be similar to other medical problems. Medical organizations have created diagnostic criteria to ease and standardize the diagnostic process especially in the first stages of the disease. Schumacher criteria were the first internationally recognized criteria for diagnosis, and introduced concepts still in use, as CDMS.
Malignant multiple sclerosis is used to describe MS patients who reach significant level of disability in a short period of time. Malignant MS cases are not common, less than 5% of patients with MS experience this type of progression.
Current standards for diagnosing multiple sclerosis (MS) are based on the 2018 revision of McDonald criteria. They rely on MRI detection of demyelinating lesions in the CNS, which are distributed in space (DIS) and in time (DIT). It is also a requirement that any possible known disease that produces demyelinating lesions is ruled out before applying McDonald's criteria.
Radiologically isolated syndrome (RIS) is a clinical situation in which a person has white matter lesions suggestive of multiple sclerosis (MS), as shown on an MRI scan that was done for reasons unrelated to MS symptoms. The nerve lesions in these people show dissemination in space with an otherwise normal neurological examination and without historical accounts of typical MS symptoms.
Anti-AQP4 diseases, are a group of diseases characterized by auto-antibodies against aquaporin 4.
↑ Navarro S, Mondéjar-Marín B, Pedrosa-Guerrero A, Pérez-Molina I, Garrido-Robres J, Alvarez-Tejerina A (2005). "[Aphasia and parietal syndrome as the presenting symptoms of a demyelinating disease with pseudotumoral lesions]". Rev Neurol. 41 (10): 601–3. PMID16288423.
↑ "Fatigue". Letchworth Garden City, United Kingdom: Multiple Sclerosis Trust.
↑ Moore H, Nair KP, Baster K, Middleton R, Paling D, Sharrack B (August 2022). "Fatigue in multiple sclerosis: A UK MS-register based study". Multiple Sclerosis and Related Disorders. 64: 103954. doi:10.1016/j.msard.2022.103954. PMID35716477.
1 2 3 The Royal College of Physicians (2004). Multiple Sclerosis. National clinical guideline for diagnosis and management in primary and secondary care. Salisbury, Wiltshire: Sarum ColourView Group. ISBN978-1-86016-182-7. Free full text (2004-08-13). Retrieved on 2007-10-01.
↑ Mathiowetz VG, Finlayson ML, Matuska KM, Chen HY, Luo P (2005). "Randomized controlled trial of an energy conservation course for persons with multiple sclerosis". Mult. Scler. 11 (5): 592–601. doi:10.1191/1352458505ms1198oa. PMID16193899. S2CID33902095.
↑ Matuska K, Mathiowetz V, Finlayson M (2007). "Use and perceived effectiveness of energy conservation strategies for managing multiple sclerosis fatigue". The American Journal of Occupational Therapy. 61 (1): 62–9. doi:10.5014/ajot.61.1.62. PMID17302106.
↑ Sepulcre J, Masdeu J, Goñi J, etal. (November 2008). "Fatigue in multiple sclerosis is associated with the disruption of frontal and parietal pathways". Mult. Scler. 15 (3): 337–44. doi:10.1177/1352458508098373. PMID18987107. S2CID2701289.
↑ Hennessey A, Robertson NP, Swingler R, Compston DA (1999). "Urinary, faecal and sexual dysfunction in patients with multiple sclerosis". J. Neurol. 246 (11): 1027–32. doi:10.1007/s004150050508. PMID10631634. S2CID30179761.
↑ Burguera-Hernández JA (2000). "[Urinary alterations in multiple sclerosis]". Revista de Neurología (in Spanish). 30 (10): 989–92. doi:10.33588/rn.3010.99371. PMID10919202.
↑ Ayuso-Peralta L, de Andrés C (2002). "[Symptomatic treatment of multiple sclerosis]". Revista de Neurología (in Spanish). 35 (12): 1141–53. doi:10.33588/rn.3512.2002385. PMID12497297.
↑ Bobholz J, Rao S (2003). "Cognitive dysfunction in multiple sclerosis: a review of recent developments". Current Opinion in Neurology. 16 (3): 283–8. doi:10.1097/00019052-200306000-00006. PMID12858063.
1 2 3 Amato MP, Ponziani G, Siracusa G, Sorbi S (October 2001). "Cognitive dysfunction in early-onset multiple sclerosis: a reappraisal after 10 years". Arch. Neurol. 58 (10): 1602–6. doi:10.1001/archneur.58.10.1602. PMID11594918.
1 2 Benedict RH, Carone DA, Bakshi R (July 2004). "Correlating brain atrophy with cognitive dysfunction, mood disturbances, and personality disorder in multiple sclerosis". J Neuroimaging. 14 (3 Suppl): 36S–45S. doi:10.1177/1051228404266267 (inactive 2024-02-28). PMID15228758.{{cite journal}}: CS1 maint: DOI inactive as of February 2024 (link)
↑ Shawaryn M, Schultheis M, Garay E, Deluca J (2002). "Assessing functional status: exploring the relationship between the multiple sclerosis functional composite and driving". Arch Phys Med Rehabil. 83 (8): 1123–9. doi:10.1053/apmr.2002.33730. PMID12161835.
↑ Rao S, Leo G, Bernardin L, Unverzagt F (1991). "Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns, and prediction". Neurology. 41 (5): 685–91. doi:10.1212/wnl.41.5.685. PMID2027484. S2CID9962959.
↑ Murray ED, Buttner N, Price BH. (2012) Depression and Psychosis in Neurological Practice. In: Neurology in Clinical Practice, 6th Edition. Bradley WG, Daroff RB, Fenichel GM, Jankovic J (eds.) Butterworth Heinemann. April 12, 2012. ISBN1437704344 | ISBN978-1437704341
↑ Leigh RJ, Averbuch-Heller L, Tomsak RL, Remler BF, Yaniglos SS, Dell'Osso LF (1994). "Treatment of abnormal eye movements that impair vision: strategies based on current concepts of physiology and pharmacology". Annals of Neurology. 36 (2): 129–41. doi:10.1002/ana.410360204. PMID8053648. S2CID23670958.
↑ Starck M, Albrecht H, Pöllmann W, Straube A, Dieterich M (1997). "Drug therapy for acquired pendular nystagmus in multiple sclerosis". J. Neurol. 244 (1): 9–16. doi:10.1007/PL00007728. PMID9007739. S2CID12333107.
↑ Jain S, Proudlock F, Constantinescu CS, Gottlob I (2002). "Combined pharmacologic and surgical approach to acquired nystagmus due to multiple sclerosis". Am. J. Ophthalmol. 134 (5): 780–2. doi:10.1016/S0002-9394(02)01629-X. PMID12429265.
↑ "The 5-year risk of MS after optic neuritis: experience of the optic neuritis treatment trial. 1997". Neurology. 57 (12 Suppl 5): S36–45. 2001. PMID11902594.
↑ Kerns RD, Kassirer M, Otis J (2002). "Pain in multiple sclerosis: a biopsychosocial perspective". Journal of Rehabilitation Research and Development. 39 (2): 225–32. PMID12051466.
↑ Solaro C, Messmer Uccelli M, Uccelli A, Leandri M, Mancardi GL (2000). "Low-dose gabapentin combined with either lamotrigine or carbamazepine can be useful therapies for trigeminal neuralgia in multiple sclerosis". Eur. Neurol. 44 (1): 45–8. doi:10.1159/000008192. hdl:11567/301010. PMID10894995. S2CID39508538.
↑ Athanasiou TC, Patel NK, Renowden SA, Coakham HB (2005). "Some patients with multiple sclerosis have neurovascular compression causing their trigeminal neuralgia and can be treated effectively with MVD: report of five cases". British Journal of Neurosurgery. 19 (6): 463–8. doi:10.1080/02688690500495067. PMID16574557. S2CID33819410.
↑ Eldridge PR, Sinha AK, Javadpour M, Littlechild P, Varma TR (2003). "Microvascular decompression for trigeminal neuralgia in patients with multiple sclerosis". Stereotactic and Functional Neurosurgery. 81 (1–4): 57–64. doi:10.1159/000075105. PMID14742965. S2CID39449873.
↑ Sandyk R, Dann LC (1995). "Resolution of Lhermitte's sign in multiple sclerosis by treatment with weak electromagnetic fields". Int. J. Neurosci. 81 (3–4): 215–24. doi:10.3109/00207459509004888. PMID7628912.
↑ O'Leary, M., Heyman, R., Erickson, J., Chancellor, M.B.: Premature ejaculation and MS: A Review, Consortium of MS Centers, http://www.mscare.org, June 2007
↑ Cardini RG, Crippa AC, Cattaneo D (2000). "Update on multiple sclerosis rehabilitation". J. Neurovirol. 6 (Suppl 2): S179–85. PMID10871810.
↑ Solmaz Asnafi et al., The Frequency of Longitudinally Extensive Transverse Myelitis in MS; A Population-Based Study, October 30, 2019, DOI: https://doi.org/10.1016/j.msard.2019.101487
↑ Bozek CB, Kastrukoff LF, Wright JM, Perry TL, Larsen TA (1987). "A controlled trial of isoniazid therapy for action tremor in multiple sclerosis". J. Neurol. 234 (1): 36–9. doi:10.1007/BF00314007. PMID3546605. S2CID23597601.
↑ Hallett M, Lindsey JW, Adelstein BD, Riley PO (1985). "Controlled trial of isoniazid therapy for severe postural cerebellar tremor in multiple sclerosis". Neurology. 35 (9): 1374–7. doi:10.1212/wnl.35.9.1374. PMID3895037. S2CID30254514.
↑ Information from the USA National library of medicine on Isoniazid
↑ Sechi GP, Zuddas M, Piredda M, Agnetti V, Sau G, Piras ML, Tanca S, Rosati G (1989). "Treatment of cerebellar tremors with carbamazepine: a controlled trial with long-term follow-up". Neurology. 39 (8): 1113–5. doi:10.1212/wnl.39.8.1113. PMID2668787. S2CID36050520.
↑ Aisen ML, Holzer M, Rosen M, Dietz M, McDowell F (1991). "Glutethimide treatment of disabling action tremor in patients with multiple sclerosis and traumatic brain injury". Arch. Neurol. 48 (5): 513–5. doi:10.1001/archneur.1991.00530170077023. PMID2021365.
↑ Mills RJ, Yap L, Young CA (2007). Mills RJ (ed.). "Treatment for ataxia in multiple sclerosis". Cochrane Database of Systematic Reviews (1): CD005029. doi:10.1002/14651858.CD005029.pub2. PMID17253537.
↑ Aisen ML, Arnold A, Baiges I, Maxwell S, Rosen M (1993). "The effect of mechanical damping loads on disabling action tremor". Neurology. 43 (7): 1346–50. doi:10.1212/wnl.43.7.1346. PMID8327136. S2CID23433712.
↑ Bittar RG, Hyam J, Nandi D, Wang S, Liu X, Joint C, Bain PG, Gregory R, Stein J, Aziz TZ (2005). "Thalamotomy versus thalamic stimulation for multiple sclerosis tremor". Journal of Clinical Neuroscience. 12 (6): 638–42. doi:10.1016/j.jocn.2004.09.008. PMID16098758. S2CID38770179.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.