Caesarean section, also known as C-section or caesarean delivery, is the surgical procedure by which one or more babies are delivered through an incision in the mother's abdomen, often performed because vaginal delivery would put the baby or mother at risk. Reasons for the operation include obstructed labor, twin pregnancy, high blood pressure in the mother, breech birth, and problems with the placenta or umbilical cord. A caesarean delivery may be performed based upon the shape of the mother's pelvis or history of a previous C-section. A trial of vaginal birth after C-section may be possible. The World Health Organization recommends that caesarean section be performed only when medically necessary. Most C-sections are performed without a medical reason, upon request by someone, usually the mother.

Childbirth, also known as labour and delivery, is the ending of pregnancy where one or more babies exits the internal environment of the mother via vaginal delivery or caesarean section. In 2019, there were about 140.11 million births globally. In the developed countries, most deliveries occur in hospitals, while in the developing countries most are home births.

The pubic symphysis is a secondary cartilaginous joint between the left and right superior rami of the pubis of the hip bones. It is in front of and below the urinary bladder. In males, the suspensory ligament of the penis attaches to the pubic symphysis. In females, the pubic symphysis is close to the clitoris. In most adults it can be moved roughly 2 mm and with 1 degree rotation. This increases for women at the time of childbirth.

A breech birth is when a baby is born bottom first instead of head first, as is normal. Around 3–5% of pregnant women at term have a breech baby. Due to their higher than average rate of possible complications for the baby, breech births are generally considered higher risk. Breech births also occur in many other mammals such as dogs and horses, see veterinary obstetrics.

External cephalic version (ECV) is a process by which a breech baby can sometimes be turned from buttocks or foot first to head first. It is a manual procedure that is recommended by national guidelines for breech presentation of a pregnancy with a single baby, in order to enable vaginal delivery. It is usually performed late in pregnancy, that is, after 36 gestational weeks, preferably 37 weeks, and can even be performed in early labour.
Labor induction is the process or treatment that stimulates childbirth and delivery. Inducing (starting) labor can be accomplished with pharmaceutical or non-pharmaceutical methods. In Western countries, it is estimated that one-quarter of pregnant women have their labor medically induced with drug treatment. Inductions are most often performed either with prostaglandin drug treatment alone, or with a combination of prostaglandin and intravenous oxytocin treatment.
Obstructed labour, also known as labour dystocia, is the baby not exiting the pelvis because it is physically block during childbirth although the uterus contracts normally. Complications for the baby include not getting enough oxygen which may result in death. It increases the risk of the mother getting an infection, having uterine rupture, or having post-partum bleeding. Long-term complications for the mother include obstetrical fistula. Obstructed labour is said to result in prolonged labour, when the active phase of labour is longer than 12 hours.

Shoulder dystocia is when, after vaginal delivery of the head, the baby's anterior shoulder gets caught above the mother's pubic bone. Signs include retraction of the baby's head back into the vagina, known as "turtle sign". Complications for the baby may include brachial plexus injury, or clavicle fracture. Complications for the mother may include vaginal or perineal tears, postpartum bleeding, or uterine rupture.
The obstetrical dilemma is a hypothesis to explain why humans often require assistance from other humans during childbirth to avoid complications, whereas most non-human primates give birth unassisted with relatively little difficulty. This occurs due to the tight fit of the fetal head to the maternal birth canal, which is additionally convoluted, meaning the head and therefore body of the infant must rotate during childbirth in order to fit, unlike in other, non-upright walking mammals. Consequently, there is a usually high incidence of cephalopelvic disproportion and obstructed labor in humans.
Caesarean delivery on maternal request (CDMR) is a caesarean section birth requested by the pregnant woman without a medical reason.

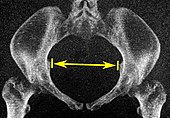
The lower circumference of the lesser pelvis is very irregular; the space enclosed by it is named the inferior aperture or pelvic outlet. It is an important component of pelvimetry.

Pubic symphysis diastasis is the separation of normally joined pubic bones, as in the dislocation of the bones, without a fracture that measures radiologically more than 10 mm. Separation of the symphysis pubis is a rare pathology associated with childbirth and has an incidence of 1 in 300 to 1 in 30,000 births. It is usually noticed after delivery but can be observed up to six months postpartum. Risk factors associated with this injury include cephalopelvic disproportion, rapid second stage of labor, epidural anesthesia, severe abduction of the thighs during delivery, or previous trauma to the pelvis. Common signs and symptoms include symphyseal pain aggravated by weight-bearing and walking, a waddling gait, pubic tenderness, and a palpable interpubic gap. Treatment for pubic symphysis diastasis is largely conservative, with treatment modalities including pelvic bracing, bed rest, analgesia, physical therapy, and in some severe cases, surgery.

Obstetrical forceps are a medical instrument used in childbirth. Their use can serve as an alternative to the ventouse method.
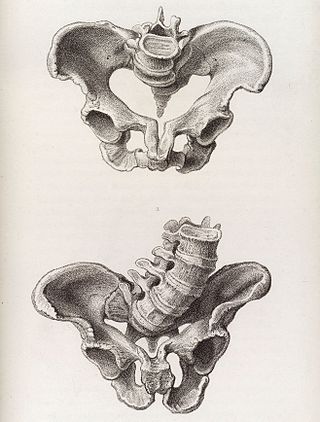
Cephalopelvic disproportion exists when the capacity of the pelvis is inadequate to allow the fetus to negotiate the birth canal. This may be due to a small pelvis, a nongynecoid pelvic formation, a large fetus, an unfavorable orientation of the fetus, or a combination of these factors. Certain medical conditions may distort pelvic bones, such as rickets or a pelvic fracture, and lead to CPD.

A vaginal delivery is the birth of offspring in mammals through the vagina. It is the most common method of childbirth worldwide. It is considered the preferred method of delivery, with lower morbidity and mortality than Caesarean sections (C-sections).

In obstetrics, the presentation of a fetus about to be born specifies which anatomical part of the fetus is leading, that is, is closest to the pelvic inlet of the birth canal. According to the leading part, this is identified as a cephalic, breech, or shoulder presentation. A malpresentation is any presentation other than a vertex presentation.
The following outline is provided as an overview of and topical guide to obstetrics:
Septic pelvic thrombophlebitis (SPT), also known as suppurative pelvic thrombophlebitis, is a rare postpartum complication which consists of a persistent postpartum fever that is not responsive to broad-spectrum antibiotics, in which pelvic infection leads to infection of the vein wall and intimal damage leading to thrombogenesis in the ovarian veins. The thrombus is then invaded by microorganisms. Ascending infections cause 99% of postpartum SPT.

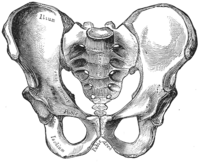
The pelvis is the lower part of the trunk, between the abdomen and the thighs, together with its embedded skeleton.
Locked twins is a rare complication of multiple pregnancy where two fetuses become interlocked during presentation before birth. It occurs in roughly 1 in 1,000 twin deliveries and 1 in 90,000 deliveries overall. Most often, locked twins are delivered via Caesarean section, given that the condition has been diagnosed early enough. The fetal mortality rate is high for the twin that presents first, with over 50% being stillborn.