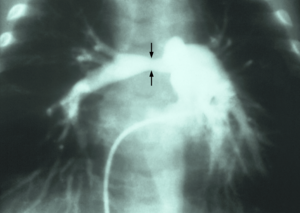
Pulmonary artery stenosis (PAS) is a narrowing of the pulmonary artery. The pulmonary artery is a blood vessel moving blood from the right side of the heart to the lungs. This narrowing can be due to many causes including infection during pregnancy, a heart defect present at birth, a problem with blood clotting in childhood or early adulthood, or a genetic change.[1] The narrowing can occur at many different points along the pulmonary artery. The specific location of stenosis indicates how severe the disease is and what treatment options someone has. Most people with high-risk PAS are neonates, a newborn child, and young children. This is because the more severe the disease the more likely it is to present with symptoms and obviously signs. With these high-risk patients, it is necessary and acceptable to treat because letting this disease persist can lead to worsening blood pressure, poor heart function, and worsening vessel disease in other parts of the body.[2]
The blood flows in a very specific and methodical way through the body. Blood that has already delivered oxygen to body returns to the right upper chamber of the heart. It then gets pumped though the tricuspid valve and into the lower right chamber. The blood is then pumped through the pulmonary valve into the pulmonary artery and toward the lungs. The blood then receives oxygen in the lungs and is transported back to the left side of the heart before being pumped to the rest of the body.[3] When the pulmonary artery, a vessel taking blood away from the heart, becomes narrow it still needs to pump the same amount of blood which causes the heart to have to pump harder. This increased force of pumping increases blood pressure on the right side of the heart and forces the heart muscle to work harder.[1]
Pulmonary artery stenosis should be differentiated from pulmonary valve stenosis. The pulmonary valve is the opening between the right heart and the pulmonary artery. Since it is right before the pulmonary artery narrowing of the valve and have similar effects to that of narrowing of the vessel itself. The most important reason to recognize the difference is because treatment varies for both. Also, the consequences of each disease long term can vary and present with other comorbid factors. Simply put, knowing specifically which of these a patient has is important to help treat them and prevent future problems.[4]
Symptoms
Pulmonary artery stenosis symptoms depend on the specific location and cause of the narrowing, though many individuals do present with similar symptoms. Common symptoms include:[5]
Other symptoms are caused by lack of oxygenated blood flow to the body. As discussed previously, blood travels through the pulmonary artery to the lungs to get oxygen. If blood has trouble getting to the lungs, the rest of the body will not receive enough oxygen. This causes individuals to present with:[5]
Dizziness
Episodes of passing out (brain not receiving enough oxygen and blood)
Inability to keep up with physical activity or not wanting to be physically active
Blue discoloration of the lips, fingers, or toes (cyanosis)
When blood cannot move from the right side of the heart to the lungs because of the narrowing, it can cause the blood to back up. This can lead to swelling in parts of the body like the hands and feet and can present similarly to right sided heart failure.[5]
Causes
Though 40% of individuals don’t have any other underlying heart problems, PAS can still occur in 2-3% of individuals with underlying heart disease they were born with:
Tetralogy of Fallot: a condition characterized by an obstruction in blood leaving the right side of the heart, enlargement in the lower right chamber of the heart, an opening between the right and left lower chambers of the heart, and mispositioned aorta.
Pulmonary atresia: a condition where the pulmonary valve does not form, and blood is unable to travel from the right side of the heart to the lungs.
Truncus arteriosus: One large vessel leaves the heart instead of two separate vessels, one from the right, one from the left.
Aortic stenosis: The valve allowing blood to leave the left side of the heart is narrowed.
Atrial septal defect: A hole between the right and left upper chambers in the heart is present allowing blood from the left to enter the right.
Ventricular septal defect: a hole between the right and left lower chambers of the heart allowing blood from the left, higher pressure side, to enter the right.
Transposition of the great vessels: A condition where the aorta and pulmonary artery swap where they receive blood from. Blood from the left side of the heart enters the pulmonary artery and goes to the lungs instead of the body and the blood from the right side of the heart (without oxygen) enters the aorta and goes to the body instead of the lungs.
Patent ductus arteriosus: the ductus arteriosus connects the pulmonary artery and aorta before birth and just after birth. In this condition the ductus does not shrink and close but remains open and causes extra blood to flow into the lungs and left side of the heart.[5]
There are also genetic and infectious causes of pulmonary artery stenosis. The most common of these are:
Williams syndrome and Alagille syndrome: mutation in the elastin gene resulting in an abnormality in the structure of the pulmonary arteries along with abnormalities in other organs.[4]
Noonan syndrome: genetic mutation in a pathway regulating what other genes are expressed.[4]
Ehlers–Danlos syndrome: mutation in collagen and other portions of connective tissue that make up parts of the body like blood vessels.[4]
Takayasu's arteritis: inflammatory disease results in damage, hardening, and occlusion to blood vessels leading to narrowing.[6]
Rubella: infection during pregnancy can lead to heart abnormalities in neonates[5]
Diagnosis
There is no immediate way to know if a child has PAS, but if an abnormal heart sounds, also known as a murmur, is heard on physical exam, further testing is ordered to evaluate the cause.
Electrocardiogram (EKG): electrical recording of the heart that can show irregular heartbeats and changes in the heart muscle.
Chest X-ray: shows shape and size of the heart and surrounding vessels.
Echocardiogram: using sound waves to get a real time picture of the heart including the muscles, valves, and vessels.
Computed Tomography (CT) Scan: using a series of x-rays to create a detailed view of the heart and vessels. Using contrast dye can allow for visualization of blood flow and any narrowing that may be present.[5][6]
Cardiac Catheterization: a procedure usually done by a heart specialist. It involves inserting a catheter (small tube) through a vessel and navigating it to the heart for better imaging and testing. Specialists can also perform treatments while the catheter is inserted.
There are currently 3 mainstays of treatment for pulmonary artery stenosis. Those are balloon angioplasty, cutting balloon angioplasty, and stenting. Prior to the development of balloon angioplasty, surgical angioplasty was the main treatment method.[4] Because of lack of efficacy, limited accessibility to certain areas of stenosis, increased risk for scarring, and a high rate of repeat stenosis, surgical angioplasty is only used if other methods fail or if surgeons are able to directly visualize the narrowing while repairing another heart defect. Some studies have shown only a 62% surgical success rate for surgical angioplasty. This would still call for other forms of treatment in about 4/10 patients while exposing them to increased risks of open surgery.[2]
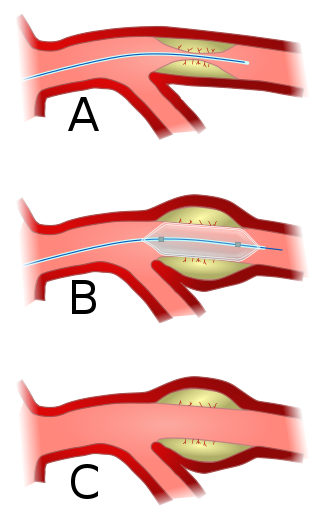
Balloon angioplasty is a less invasive method to help expand the diameter of a vessel to improve narrowing. In this treatment a catheter with a balloon on the end is inserted into a larger, peripheral vessel and moved to the area of narrowing. The goal of this treatment method is to tear two of the three layers of the artery which increases both the vessel’s diameter and the flow of blood throw the vessel. Initially a soft balloon was used but only about 60% of patients had at least a 50% increase in blood flow. This is similar is efficacy to surgical angioplasty with a large reduction in associated risks. Later on a stiffer balloon was used and efficacy improved to 72% with no increase in associated risks.[4]
After the procedure is performed, there are several key factors that help determine if the procedure was successful/will remain successful. These are: 1) evidence on imaging or tissue sampling of tearing of the vessel wall, 2) larger ratio of balloon diameter to vessel diameter, 3) cause of the pulmonary artery stenosis (surgically caused stenosis is more likely to be successful), and 4) location of the narrowing as vessels further from the heart are more elastic and more difficult to treat with just balloon angioplasty.[4]
One of the major concerns with balloon angioplasty is the rate of restenosis. Even when there is evidence of tearing of the vessel wall, the rate of restenosis (or repeat narrowing) is between 15-44%. Studies have also shown the rate of restenosis increases as time from the procedure increases. Rates of complications overall are estimated around 22%, with 10% being higher risk complications. Other complications from this procedure are likely from too much damage to vessels and include full vessel tears, deep vein thrombosis (clot in the vessel), complete rupture of the pulmonary artery, and pulmonary edema (fluid in the lungs causing worsening breathing).[4]
The major reasons for simple balloon angioplasty failure are inability to tear the vessel wall, restenosis, areas of narrowing due to compression by another internal body part rather than issues with the vessel itself. To help counteract the first, cutting balloon angioplasty was invented. This method utilizes balloons with a blade that can cut through vessel walls rather than simply causing vessel wall tearing via crushing/expansion of the balloon. When the balloon is not inflated the blades are protected inside the balloon folds, ensuring they will not accidentally damage other vessels.[4] After the use of the cutting balloon, a larger, higher-pressure balloon can be used to improve efficacy. Multicenter studies show the same safety profiles for simple versus cutting balloon angioplasty with rates of adverse effects of 2% and 3% respectively. When a high-pressure balloon was used after cutting balloon angioplasty the rate of effectiveness increased from 52% to 85%.[2] It should also be noted cutting balloon angioplasty provides more areas of vessel damage especially in vessels further from the heart. Overall it is noted that cutting balloon angioplasty has similar complications and restenosis rates as simple, but offers a more effective treatment as well as being a better option for smaller areas of stenosis.[4]
To solve the latter two problems of restenosis and external compression of a vessel, metal stents were introduced. These stents would be deployed via a catheter. They could be expanded at the site specifically. The stents form a rigid structure that would hold in place and remain inside the vessel. Newer studies have shown successful dilation in 90% of patients on average with some newer studies indicating a 100% success rate. The benefits of these stents is not only their long term efficacy but the prevention of long term heart disease. Stents helped improve right sided heart pressures, blood flow to the lungs, and pressure difference between the right and left sides of the heart. Stents have been noted to be sustainable with replacement for up to 15 years, much longer than if a patient received any sort of balloon angioplasty. Stents have the lowest rate of restenosis at 2-3%.[4]
Stents also allowed for normal growth of the vessels during childhood and adolescent years, and did not damage the heart or vasculature. Though, because young children grow very rapidly, 30-50% of children who received stents did require replacement with a larger stent in the first 2 years of placement. Complication rates are around 12% and include misplacement due to blood flow over time, vessel damage from the metal stent moving, or formation of a clot on the stent leading to blocked blood flow. Because of these concerns and necessary removal of the stent if these were to occur, a patient would need to have the stent monitored frequently after placement.[4]
Another concern with stents is fracturing, or breaking, of the stent due to repetitive pressure. One study early in stent usage for pulmonary artery stenosis showed fracturing in about 21% of patients. 80% of these patients then had significant vessel obstruction because of the break. With continual improvements to stents, the newer data reveals a 13% adverse event rate with only 1.2% being major adverse events, such as a fracture leading to major vessel obstruction. Success rate for dilation in this study was 99%, much higher than the 72% for cutting balloon angioplasty. Of note, studies have shown the adverse event rate decreases as the patient’s age increases, likely due to less significant growth in the vessel. Some studies do indicate the need for replacement of a stent as high as 43%, but this rate does increase over time. Currently the recommendations are to treat younger patients with balloon angioplasty until they are older and the risk for metal stents is significantly reduced.[2] Future advancement for bioresorbable stents (stents that would be absorbed by the body) is in the works as this would reduce the need to continually replace stents in growing humans.[2][4]
Related Research Articles
Angioplasty, also known as balloon angioplasty and percutaneous transluminal angioplasty (PTA), is a minimally invasive endovascular procedure used to widen narrowed or obstructed arteries or veins, typically to treat arterial atherosclerosis. A deflated balloon attached to a catheter is passed over a guide-wire into the narrowed vessel and then inflated to a fixed size. The balloon forces expansion of the blood vessel and the surrounding muscular wall, allowing an improved blood flow. A stent may be inserted at the time of ballooning to ensure the vessel remains open, and the balloon is then deflated and withdrawn. Angioplasty has come to include all manner of vascular interventions that are typically performed percutaneously.
Interventional radiology (IR) is a medical specialty that performs various minimally-invasive procedures using medical imaging guidance, such as x-ray fluoroscopy, computed tomography, magnetic resonance imaging, or ultrasound. IR performs both diagnostic and therapeutic procedures through very small incisions or body orifices. Diagnostic IR procedures are those intended to help make a diagnosis or guide further medical treatment, and include image-guided biopsy of a tumor or injection of an imaging contrast agent into a hollow structure, such as a blood vessel or a duct. By contrast, therapeutic IR procedures provide direct treatment—they include catheter-based medicine delivery, medical device placement, and angioplasty of narrowed structures.
A coronary catheterization is a minimally invasive procedure to access the coronary circulation and blood filled chambers of the heart using a catheter. It is performed for both diagnostic and interventional (treatment) purposes.
dextro-Transposition of the great arteries is a potentially life-threatening birth defect in the large arteries of the heart. The primary arteries are transposed.
Mitral stenosis is a valvular heart disease characterized by the narrowing of the opening of the mitral valve of the heart. It is almost always caused by rheumatic valvular heart disease. Normally, the mitral valve is about 5 cm2 during diastole. Any decrease in area below 2 cm2 causes mitral stenosis. Early diagnosis of mitral stenosis in pregnancy is very important as the heart cannot tolerate increased cardiac output demand as in the case of exercise and pregnancy. Atrial fibrillation is a common complication of resulting left atrial enlargement, which can lead to systemic thromboembolic complications such as stroke.
Restenosis is the recurrence of stenosis, a narrowing of a blood vessel, leading to restricted blood flow. Restenosis usually pertains to an artery or other large blood vessel that has become narrowed, received treatment to clear the blockage and subsequently become renarrowed. This is usually restenosis of an artery, or other blood vessel, or possibly a vessel within an organ.
Stenosis is the abnormal narrowing of a blood vessel or other tubular organ or structure such as foramina and canals. It is also sometimes called a stricture.
Interventional cardiology is a branch of cardiology that deals specifically with the catheter based treatment of structural heart diseases. Andreas Gruentzig is considered the father of interventional cardiology after the development of angioplasty by interventional radiologist Charles Dotter.
Intravascular ultrasound (IVUS) or intravascular echocardiography is a medical imaging methodology using a specially designed catheter with a miniaturized ultrasound probe attached to the distal end of the catheter. The proximal end of the catheter is attached to computerized ultrasound equipment. It allows the application of ultrasound technology, such as piezoelectric transducer or CMUT, to see from inside blood vessels out through the surrounding blood column, visualizing the endothelium of blood vessels.
Cardiac catheterization is the insertion of a catheter into a chamber or vessel of the heart. This is done both for diagnostic and interventional purposes.
Pulmonary valve stenosis (PVS) is a heart valve disorder. Blood going from the heart to the lungs goes through the pulmonary valve, whose purpose is to prevent blood from flowing back to the heart. In pulmonary valve stenosis this opening is too narrow, leading to a reduction of flow of blood to the lungs.
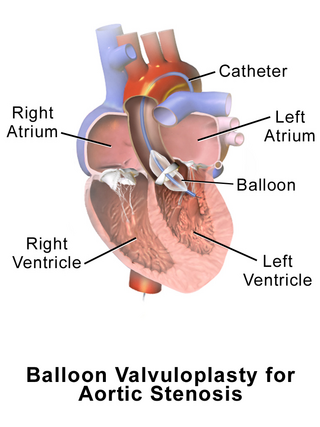
Aortic valvuloplasty, also known as balloon aortic valvuloplasty (BAV), is a procedure used to improve blood flow through the aortic valve in conditions that cause aortic stenosis, or narrowing of the aortic valve. It can be performed in various patient populations including fetuses, newborns, children, adults, and pregnant women. The procedure involves using a balloon catheter to dilate the narrowed aortic valve by inflating the balloon.
Percutaneous coronary intervention (PCI) is a non-surgical procedure used to treat narrowing of the coronary arteries of the heart found in coronary artery disease. The process involves combining coronary angioplasty with stenting, which is the insertion of a permanent wire-meshed tube that is either drug eluting (DES) or composed of bare metal (BMS). The stent delivery balloon from the angioplasty catheter is inflated with media to force contact between the struts of the stent and the vessel wall, thus widening the blood vessel diameter. After accessing the blood stream through the femoral or radial artery, the procedure uses coronary catheterization to visualise the blood vessels on X-ray imaging. After this, an interventional cardiologist can perform a coronary angioplasty, using a balloon catheter in which a deflated balloon is advanced into the obstructed artery and inflated to relieve the narrowing; certain devices such as stents can be deployed to keep the blood vessel open.
Drug-eluting stents (DES) are a type of stent and a medical drug delivery device used in the treatment of various medical conditions, with its primary application being the treatment of coronary artery disease (CAD).
The history of invasive and interventional cardiology is complex, with multiple groups working independently on similar technologies. Invasive and interventional cardiology is currently closely associated with cardiologists, though the development and most of its early research and procedures were performed by diagnostic and interventional radiologists.
Lutembacher's syndrome is a very rare form of congenital heart disease that affects one of the chambers of the heart as well as a valve. It is commonly known as both congenital atrial septal defect (ASD) and acquired mitral stenosis (MS). Congenital atrial septal defect refers to a hole being in the septum or wall that separates the two atria; this condition is usually seen in fetuses and infants. Mitral stenosis refers to mitral valve leaflets sticking to each other making the opening for blood to pass from the atrium to the ventricles very small. With the valve being so small, blood has difficulty passing from the left atrium into the left ventricle. Septal defects that may occur with Lutembacher's syndrome include: Ostium primum atrial septal defect or ostium secundum which is more prevalent.
A coronary stent is a tube-shaped device placed in the coronary arteries that supply blood to the heart, to keep the arteries open in the treatment of coronary heart disease. It is used in a procedure called percutaneous coronary intervention (PCI). Coronary stents are now used in more than 90% of PCI procedures. Stents reduce angina and have been shown to improve survival and decrease adverse events in an acute myocardial infarction.
The following outline is provided as an overview of and topical guide to cardiology, the branch of medicine dealing with disorders of the human heart. The field includes medical diagnosis and treatment of congenital heart defects, coronary artery disease, heart failure, valvular heart disease and electrophysiology. Physicians who specialize in cardiology are called cardiologists.
Congenital stenosis of vena cava is a congenital anomaly in which the superior vena cava or inferior vena cava has an aberrant interruption or coarctation.
Balloon pulmonary angioplasty (BPA) is an emerging minimally invasive procedure to treat chronic thromboembolic pulmonary hypertension (CTEPH) in people who are not suitable for pulmonary thromboendarterectomy (PTE) or still have residual pulmonary hypertension and areas of narrowing in the pulmonary arterial tree following previous PTE.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.