
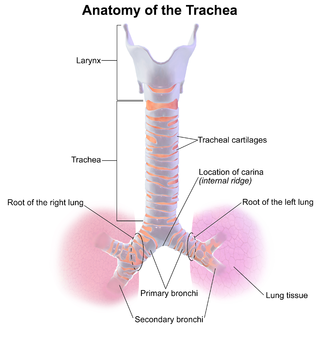
The trachea, also known as the windpipe, is a cartilaginous tube that connects the larynx to the bronchi of the lungs, allowing the passage of air, and so is present in almost all animals with lungs. The trachea extends from the larynx and branches into the two primary bronchi. At the top of the trachea the cricoid cartilage attaches it to the larynx. The trachea is formed by a number of horseshoe-shaped rings, joined together vertically by overlying ligaments, and by the trachealis muscle at their ends. The epiglottis closes the opening to the larynx during swallowing.

Tracheal intubation, usually simply referred to as intubation, is the placement of a flexible plastic tube into the trachea (windpipe) to maintain an open airway or to serve as a conduit through which to administer certain drugs. It is frequently performed in critically injured, ill, or anesthetized patients to facilitate ventilation of the lungs, including mechanical ventilation, and to prevent the possibility of asphyxiation or airway obstruction.

Mechanical ventilation, assisted ventilation or intermittent mandatory ventilation (IMV), is the medical term for using a machine called a ventilator to fully or partially provide artificial ventilation. Mechanical ventilation helps move air into and out of the lungs, with the main goal of helping the delivery of oxygen and removal of carbon dioxide. Mechanical ventilation is used for many reasons, including to protect the airway due to mechanical or neurologic cause, to ensure adequate oxygenation, or to remove excess carbon dioxide from the lungs. Various healthcare providers are involved with the use of mechanical ventilation and people who require ventilators are typically monitored in an intensive care unit.

Croup, also known as laryngotracheobronchitis, is a type of respiratory infection that is usually caused by a virus. The infection leads to swelling inside the trachea, which interferes with normal breathing and produces the classic symptoms of "barking/brassy" cough, inspiratory stridor and a hoarse voice. Fever and runny nose may also be present. These symptoms may be mild, moderate, or severe. Often it starts or is worse at night and normally lasts one to two days.

Laryngoscopy is endoscopy of the larynx, a part of the throat. It is a medical procedure that is used to obtain a view, for example, of the vocal folds and the glottis. Laryngoscopy may be performed to facilitate tracheal intubation during general anaesthesia or cardiopulmonary resuscitation or for surgical procedures on the larynx or other parts of the upper tracheobronchial tree.

The epiglottis is a leaf-shaped flap in the throat that prevents food and water from entering the trachea and the lungs. It stays open during breathing, allowing air into the larynx. During swallowing, it closes to prevent aspiration of food into the lungs, forcing the swallowed liquids or food to go along the esophagus toward the stomach instead. It is thus the valve that diverts passage to either the trachea or the esophagus.
A tracheal tube is a catheter that is inserted into the trachea for the primary purpose of establishing and maintaining a patent airway and to ensure the adequate exchange of oxygen and carbon dioxide.

Respiratory arrest is a medical condition caused by apnea or respiratory dysfunction severe enough it will not sustain the body. Prolonged apnea refers to a patient who has stopped breathing for a long period of time. If the heart muscle contraction is intact, the condition is known as respiratory arrest. An abrupt stop of pulmonary gas exchange lasting for more than five minutes may permanently damage vital organs, especially the brain. Lack of oxygen to the brain causes loss of consciousness. Brain injury is likely if respiratory arrest goes untreated for more than three minutes, and death is almost certain if more than five minutes.

Epiglottitis is the inflammation of the epiglottis—the flap at the base of the tongue that prevents food entering the trachea (windpipe). Symptoms are usually rapid in onset and include trouble swallowing which can result in drooling, changes to the voice, fever, and an increased breathing rate. As the epiglottis is in the upper airway, swelling can interfere with breathing. People may lean forward in an effort to open the airway. As the condition worsens, stridor and bluish skin may occur.
Tracheitis is an inflammation of the trachea. Although the trachea is usually considered part of the lower respiratory tract, in ICD-10 tracheitis is classified under "acute upper respiratory infections".

Smoke inhalation is the breathing in of harmful fumes through the respiratory tract. This can cause smoke inhalation injury which is damage to the respiratory tract caused by chemical and/or heat exposure as well as possible systemic toxicity after smoke inhalation. Smoke inhalation can occur from fires of various sources such as residential, vehicle, and wildfires. Morbidity and mortality rates in fire victims with burns are increased in those with smoke inhalation injury. Victims of smoke inhalation injury can present with cough, difficulty breathing, low oxygen saturation, smoke debris and/or burns on the face. Smoke inhalation injury can affect the upper respiratory tract, usually due to heat exposure, or the lower respiratory tract, usually due to exposure to toxic fumes. Initial treatment includes taking the victim away from the fire and smoke, giving 100% oxygen at a high flow through a face mask, and checking the victim for injuries to the body. Treatment for smoke inhalation injury is largely supportive with varying degrees of consensus on benefits of specific treatments.

The Combitube—also known as the esophageal tracheal airway or esophageal tracheal double-lumen airway—is a blind insertion airway device (BIAD) used in the pre-hospital and emergency setting. It is designed to provide an airway to facilitate the mechanical ventilation of a patient in respiratory distress.
Subglottic stenosis is a congenital or acquired narrowing of the subglottic airway. It can be congenital, acquired, iatrogenic, or very rarely, idiopathic. It is defined as the narrowing of the portion of the airway that lies between the vocal cords and the lower part of the cricoid cartilage. In a normal infant, the subglottic airway is 4.5-5.5 millimeters wide, while in a premature infant, the normal width is 3.5 millimeters. Subglottic stenosis is defined as a diameter of under 4 millimeters in an infant. Acquired cases are more common than congenital cases due to prolonged intubation being introduced in the 1960s. It is most frequently caused by certain medical procedures or external trauma, although infections and systemic diseases can also cause it.

Laryngotracheal stenosis refers to abnormal narrowing of the central air passageways. This can occur at the level of the larynx, trachea, carina or main bronchi. In a small number of patients narrowing may be present in more than one anatomical location.

Bronchoscopy is an endoscopic technique of visualizing the inside of the airways for diagnostic and therapeutic purposes. An instrument (bronchoscope) is inserted into the airways, usually through the nose or mouth, or occasionally through a tracheostomy. This allows the practitioner to examine the patient's airways for abnormalities such as foreign bodies, bleeding, tumors, or inflammation. Specimens may be taken from inside the lungs. The construction of bronchoscopes ranges from rigid metal tubes with attached lighting devices to flexible optical fiber instruments with realtime video equipment.

Tracheobronchial injury is damage to the tracheobronchial tree. It can result from blunt or penetrating trauma to the neck or chest, inhalation of harmful fumes or smoke, or aspiration of liquids or objects.
Double aortic arch is a relatively rare congenital cardiovascular malformation. DAA is an anomaly of the aortic arch in which two aortic arches form a complete vascular ring that can compress the trachea and/or esophagus. Most commonly there is a larger (dominant) right arch behind and a smaller (hypoplastic) left aortic arch in front of the trachea/esophagus. The two arches join to form the descending aorta which is usually on the left side. In some cases the end of the smaller left aortic arch closes and the vascular tissue becomes a fibrous cord. Although in these cases a complete ring of two patent aortic arches is not present, the term ‘vascular ring’ is the accepted generic term even in these anomalies.
Advanced airway management is the subset of airway management that involves advanced training, skill, and invasiveness. It encompasses various techniques performed to create an open or patent airway – a clear path between a patient's lungs and the outside world.

Intubation granuloma is a benign growth of granulation tissue in the larynx or trachea, which arises from tissue trauma due to endotracheal intubation. This medical condition is described as a common late complication of tracheal intubation, specifically caused by irritation to the mucosal tissue of the airway during insertion or removal of the patient's intubation tube.
Negative-pressure pulmonary edema (NPPE), also known as Postobstructive Pulmonary Edema, is a clinical phenomenon that results from the generation of large negative pressures in the airways during attempted inspiration against some form of obstruction of the upper airways. The most common reported cause of NPPE reported in adults is laryngospasm, while the most implicated causes in children are infectious croup and epiglottitis. The large negative pressures created in the airways by inhalation against an upper airway obstruction can lead to fluid being drawn from blood vessels supplying the lungs into the alveoli, causing pulmonary edema and impaired ability for oxygen exchange (hypoxemia). The main treatment for NPPE is supportive care in an intensive care unit and can be fatal without intervention.