This article's lead sectionmay be too short to adequately summarize the key points. Please consider expanding the lead to provide an accessible overview of all important aspects of the article.(November 2025)
Medical condition
Underweight
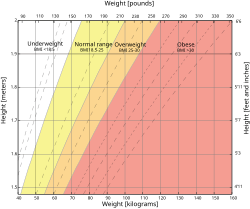
The underweight range according to the body mass index (BMI) is the white area on the chart.
Underweight is a term describing a person whose body weight is considered too low to be healthy. The definition usually refers to people with a body mass index (BMI) of under 18.5 or a weight 15% to 20% below that normal for their age and height group. While obesity is a major public health concern in many developed nations, being underweight can also carry significant health risks and is a primary cause of mortality in developing countries.
The body mass index, a ratio of a person's weight to their height, has traditionally been used to assess the health of a person as it pertains to weight: under the cut-off point at a BMI of 18.5, a person is considered underweight.[2] The calculation is given by the mass per height squared, with results usually given in kg/m^2 (for an approximate conversion from lb/in^2, divide by 703). Another measure of underweight is through comparison to the average weight of a cohort of people of a similar age and height: people who are at least 15% to 20% below the average weight for the group are considered underweight.[3]
Body fat percentage has been suggested as another way to assess whether a person is underweight. Unlike the body mass index, which is a proxy measurement, the body fat percentage takes into account the difference in composition between adipose tissue (fat cells) and muscle tissue and their different roles in the body.[4] The American Council on Exercise defines the amount of essential fat, below which a person is underweight, as 10–13% for women and 2–5% for men.[5] The greater amount of essential body fat in women supports reproductive function.[citation needed]
Prevalence
Using the body mass index as a measure of weight-related health, with data from 2014, age-standardised global prevalence of underweight in women and men were 9.7% and 8.8%, respectively. These values were lower than what was reported for 1975 as 14.6% and 13.8%, respectively, indicating a worldwide reduction in the extent of undernutrition.[6]
A common belief is that healthy underweight individuals can ‘eat what they want’ and then burn it off either by high levels of activity or elevated metabolism. It has been shown, however, that individuals with BMI < 18.5 eat about 12% less calories than individuals with normal BMI (21.5 to 25) and they are 23% less physically active (by accelerometry).[17] Underweight people tend to have low appetites and typically eat little, sporadically or infrequently.[citation needed]
Problems
Being underweight can be a symptom of an underlying condition, in which case it is secondary. Unexplained weight loss may require a professional medical diagnosis by a physician.[18]
Being underweight can also cause other conditions, in which case it is primary. Severely underweight individuals may have poor physical stamina and a weak immune system, leaving them open to infection. According to Robert E. Black of the Johns Hopkins School of Public Health (JHSPH), "Underweight status ... and micronutrient deficiencies also cause decreases in immune and non-immune host defenses, and should be classified as underlying causes of death if followed by infectious diseases that are the terminal associated causes."[19] People who are malnourished raise special concerns, as not only gross caloric intake may be inadequate, but also intake and absorption of other vital nutrients, especially essential amino acids and micronutrients such as vitamins and minerals.[citation needed]
Malnourishment can also cause anemia and hair loss.
Being underweight is an established[21] risk factor for osteoporosis, even for young people. This is seen in individuals suffering from relative energy deficiency in sport, formerly known as female athlete triad: when disordered eating or excessive exercise cause amenorrhea, hormone changes during ovulation leads to loss of bone mineral density.[22][23] After this low bone mineral density causes the first spontaneous fractures, the damage is often irreversible.
Although being underweight has been reported to increase mortality at rates comparable to that seen in morbidly obese people,[24] the effect is much less drastic when restricted to non-smokers with no history of disease,[25] suggesting that smoking and disease-related weight loss are the leading causes of the observed effect.
Treatment
Diet
Underweight individuals may be advised to gain weight by increasing calorie intake. This can be done by eating a sufficient volume of sufficiently calorie-dense foods.[26][27][28] Body weight may also be increased through the consumption of liquid nutritional supplements.[29]
Exercise
Another way for underweight people to gain weight is by exercising, since muscle hypertrophy increases body mass. Weight lifting exercises are effective in helping to improve muscle tone as well as helping with weight gain.[30] Weight lifting has also been shown to improve bone mineral density,[31] which underweight people are more likely to lack.[32]
Exercise is catabolic, which results in a brief reduction in mass. However, during recovery, anabolic overcompensation causes the muscles to grow, which results in an overall increase in mass. This can happen through an increase in muscle proteins, or through enhanced storage of glycogen in muscles.[citation needed] Exercise can also help stimulate the appetite of a person who is not inclined to eat.
↑Hira, S. K.; H. L. Dupont; D. N. Lanjewar; Y. N. Dholakia (1998). "Severe weight loss: the predominant clinical presentation of tuberculosis in patients with HIV infection in India". National Medical Journal of India. 11 (6): 256–58. PMID10083790.
↑Gjesdal; Halse, JI; Eide, GE; Brun, JG; Tell, GS (2008). "Impact of lean mass and fat mass on bone mineral density: the Hordaland Health Study". Maturitas. 59 (2): 191–200. doi:10.1016/j.maturitas.2007.11.002. PMID18221845.
↑Nattiv; Agostini, R; Drinkwater, B; Yeager, KK (1994). "The female athlete triad. The inter-relatedness of disordered eating, amenorrhea, and osteoporosis". Clinics in Sports Medicine. 13 (2): 405–18. doi:10.1016/S0278-5919(20)30338-0. PMID8013041.
↑Wilson; Wolman, RL (1994). "Osteoporosis and fracture complications in an amenorrhoeic athlete". British Journal of Rheumatology. 33 (5): 480–1. doi:10.1093/rheumatology/33.5.480. PMID8173855.
↑"Healthy Weight Gain". Children's Hospital Boston, Center for Young Women's Health. Archived from the original on July 31, 2013. Retrieved October 23, 2010.
↑"Men's Health". Men's Health. Archived from the original on September 29, 2011. Retrieved October 23, 2010.
↑Gleeson, Peggy; Elizabeth J. Protas; Adrian D. Leblanc; Victor S. Schneider; Harlan J. Evans (February 1990). "Effects of weight lifting on bone mineral density in premenopausal women". Journal of Bone and Mineral Research. 5 (2): 153–158. doi:10.1002/jbmr.5650050208. PMID2316403. S2CID72034011.
↑Coin, A.; G. Sergi; P. Benincà; L. Lupoli; G. Cinti; L. Ferrara; G. Benedetti; G. Tomasi; C. Pisent; G. Enzi (2000). "Bone Mineral Density and Body Composition in Underweight and Normal Elderly Subjects". Osteoporosis International. 11 (12): 1043–1050. doi:10.1007/s001980070026. PMID11256896. S2CID1298271.
↑Homnick, Douglas N. (2005). "Long-term trial of cyproheptadine as an appetite stimulant in cystic fibrosis". Pediatric Pulmonology. 40 (3): 251–256. doi:10.1002/ppul.20265. PMID16015665. S2CID22837100.
This page is based on this Wikipedia article Text is available under the CC BY-SA 4.0 license; additional terms may apply. Images, videos and audio are available under their respective licenses.